The Peptide Discovered in Gastric Juice and Studied for Tissue Repair
Disclaimer: Information provided is for research and educational purposes only. BPC-157 is not approved by the FDA or any regulatory agency for human use.
BPC-157 (Body Protection Compound 157) is a synthetic peptide of 15 amino acids, derived from a protein fragment found in human gastric juice. Discovered in 1993, it has shown broad tissue-repair effects in preclinical models, including muscle, tendon, nerve, and gastrointestinal healing.¹ ²
Laboratory data indicate BPC-157 promotes healing in muscles, tendons, nerves, and the gastrointestinal tract, acting via angiogenesis, modulation of the nitric-oxide system, and anti-inflammatory pathways.² ³
Primary Research: Rodent models of GI, musculoskeletal, neuroprotection
Chemical Structure & Origin
Named for its Body Protection Compound origin and its position as fragment number 157, BPC-157’s 15-amino-acid sequence confers unusual stability—even in the acidic stomach environment⁴.
BPC-157 peptide structure and amino acid sequence
Discovery of BPC-157 and Research Milestones
In 1993, Dr. Predrag Sikiric and colleagues at the University of Zagreb first described BPC-157 in Journal of Physiology-Paris, detailing its stomach-stress organoprotection hypothesis and beneficial effects in rodent gastric-injury models⁴. Their isolation of BPC-157 from human gastric juice protein laid the foundation for decades of follow-up work on tissue regeneration and organ protection.
Year
Study & Source
Key Finding
1993
Sikiric P. et al., J. Physiol.-Paris (PMID 8298609)⁴
Ulcer healing, organoprotection
1997
Sikiric P. et al., Curr. Pharm. Des. (PMID 23755725)²
NO-system modulation, blood-pressure effects
2003
Staresinic M. et al., J. Orthop. Res. (PMID 14554208)⁵
Accelerated Achilles tendon repair
2014
Sikiric P. et al., Curr. Pharm. Des. (PMID 23755725)²
Broad healing across multiple injury models
Note: All evidence to date is from animal or in vitro models; human clinical trials are pending.
How BPC-157 Differs From Other Peptides
Peptide
Main Use
Oral?
Key Difference
BPC-157
Multi-tissue repair
Yes
Stable in GI tract; broad activity
TB-500
Soft tissue repair
Yes
Targets actin, cell migration
GHK-Cu
Skin & cosmetic
No
Copper-binding; collagen stimulation
Conclusion & Key Takeaways
BPC-157 is a research peptide discovered in 1993 that shows broad healing potential in preclinical models. Its oral stability and multi-system effects make it unique among peptides, but clinical approval and human data are still pending.
FAQs About BPC-157
Who discovered BPC-157?
Dr. Predrag Sikiric and his team at the University of Zagreb, Croatia, in 1993⁴.
Is BPC-157 natural?
It’s a synthetic fragment based on a gastric-juice protein; it does not occur independently in the body.
Is BPC-157 FDA-approved?
No—BPC-157 remains investigational and is not approved by any regulatory agency.
Where can I learn more?
Read our in-depth history of BPC-157 for original studies and timelines.
Kowalski, Ł., et al. “Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review.” Pharmaceuticals 18, no. 2 (2025): 185. https://doi.org/10.3390/ph18020185
Chang, C. H., et al. “Oral Stable Gastric Pentadecapeptide BPC 157 Therapy in Muscle and Tendon Healing.” Pharmacological Reports 72, no. 1 (2020): 206–12
Sikiric, P., et al. “A New Gastric Juice Peptide, BPC. An Overview of the Stomach-Stress-Organoprotection Hypothesis and Beneficial Effects of BPC.” Journal of Physiology-Paris 87, no. 5 (1993): 313–27. PMID 8298609 https://pubmed.ncbi.nlm.nih.gov/8298609/
Staresinic, M., et al. “Gastric Pentadecapeptide BPC 157 Accelerates Healing of Transected Rat Achilles Tendon and In Vitro Stimulates Tendocyte Growth.” Journal of Orthopaedic Research 21, no. 6 (2003): 976–83. PMID 14554208 https://pubmed.ncbi.nlm.nih.gov/14554208/
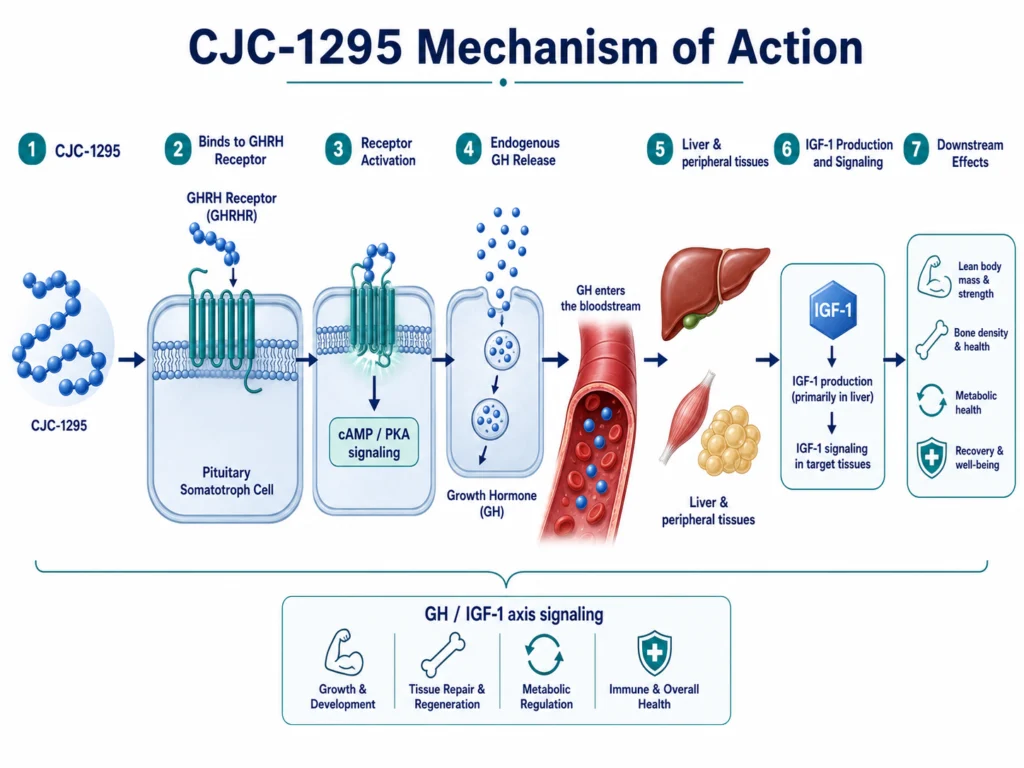
CJC-1295 is a synthetic analog of growth-hormone–releasing hormone (GHRH), studied for its ability to activate the GHRH receptor and stimulate downstream growth hormone (GH) and IGF-1 signaling.¹²
One of the most common points of confusion is the difference between CJC-1295 with DAC and CJC-1295 No DAC. Both terms are widely used in research peptide discussions, but they do not always refer to the same molecule.
This article explains the key differences between CJC-1295 DAC and No DAC, including structure, half-life, signaling pattern, research use, and safety considerations.
CJC-1295 DAC vs. No DAC: Quick Comparison
Feature
CJC-1295 with DAC
CJC-1295 No DAC / Modified GRF (1-29)
Core identity
Long-acting GHRH analog
Short-acting GHRH analog
DAC present?
Yes
No
Albumin binding
Yes — covalent albumin binding
No DAC-mediated albumin binding
Half-life
Approximately 5.8–8.1 days in human studies²
Much shorter; closer to modified GHRH fragment behavior
Signaling pattern
Sustained GH/IGF-1 stimulation
Shorter, more pulsatile GHRH-like stimulation
Main research focus
Long-duration GH-axis activation
Short-duration GH pulse modeling
Key distinction
Extended duration through DAC
Faster clearance without DAC
What Does “DAC” Mean?
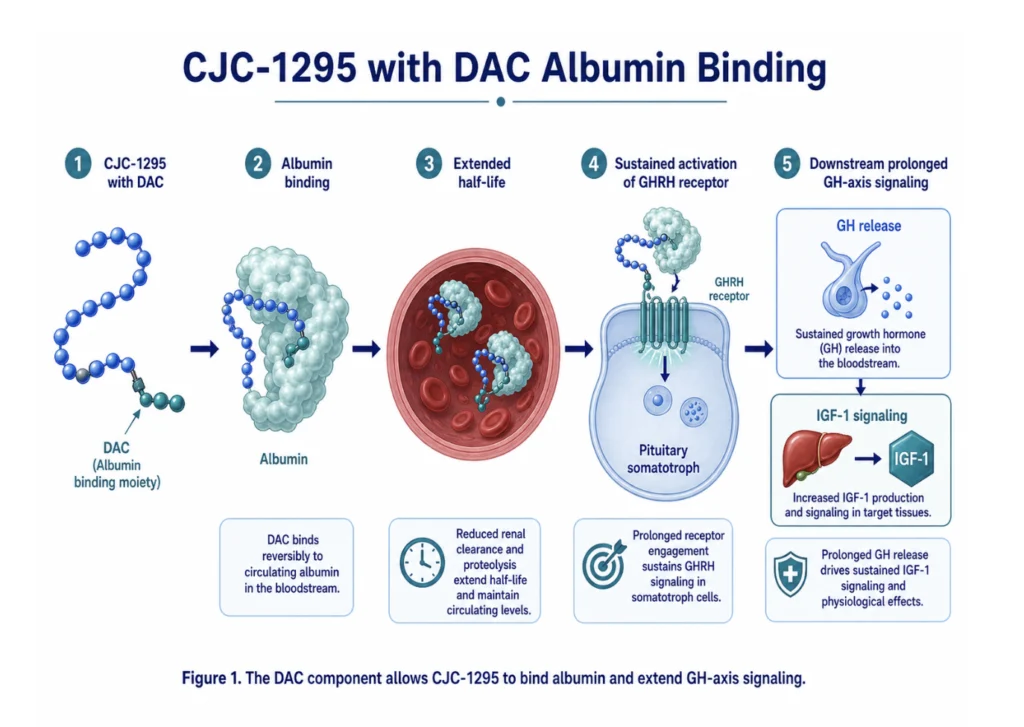
DAC stands for drug affinity complex. In CJC-1295, the DAC component allows the peptide to bind covalently to circulating albumin after administration.²³
Albumin is a long-lived blood protein. By attaching to albumin, CJC-1295 remains active much longer than native GHRH or shorter GHRH analogs. This albumin-binding mechanism is the core reason CJC-1295 with DAC has a much longer half-life.
In one clinical study, CJC-1295 produced dose-dependent increases in GH for six days or more and IGF-1 increases for nine to eleven days after a single administration. The estimated half-life was 5.8–8.1 days.²
Why it matters: DAC changes the entire pharmacokinetic profile. It turns CJC-1295 from a short-acting GHRH analog into a long-acting GH-axis research compound.
What Is CJC-1295 with DAC?
CJC-1295 with DAC is the molecule most accurately referred to as CJC-1295 in the scientific literature. It is a modified GHRH(1-29) analog designed to resist enzymatic breakdown and extend duration of action through albumin binding.¹²
Figure 1. The DAC component allows CJC-1295 to bind albumin and extend GH-axis signaling.
Key features of CJC-1295 DAC
CJC-1295 with DAC:
Activates the GHRH receptor on pituitary somatotroph cells
Stimulates endogenous GH release
Increases downstream IGF-1 signaling
Binds to albumin through the DAC structure
Produces sustained GH/IGF-1 effects over multiple days²³
Because of this extended exposure, CJC-1295 DAC is usually discussed in research contexts focused on longer-duration GH-axis activation rather than short GH pulses.
What Is CJC-1295 No DAC?
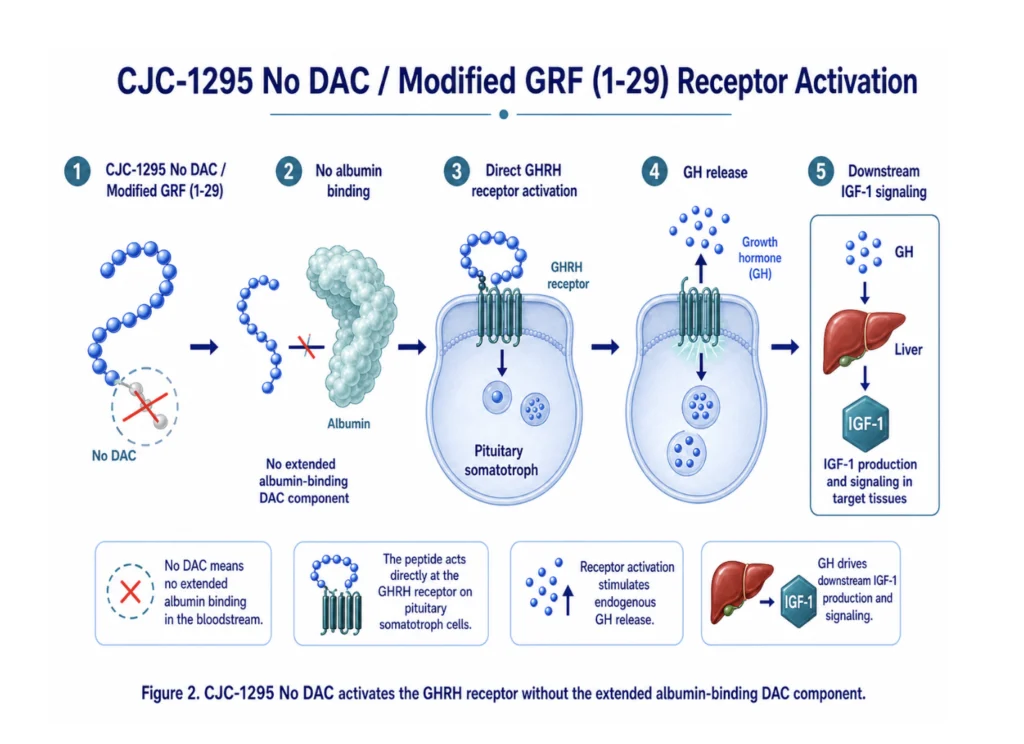
“CJC-1295 No DAC” is a common market term, but it is not always chemically precise. In many contexts, it refers to Modified GRF (1-29) — a tetrasubstituted analog of the first 29 amino acids of GHRH.
Like CJC-1295 DAC, No DAC compounds are designed to activate the GHRH receptor. The major difference is that they lack the albumin-binding DAC extension.
Figure 2. CJC-1295 No DAC activates the GHRH receptor without the extended albumin-binding DAC component.
Key features of CJC-1295 No DAC
CJC-1295 No DAC / Modified GRF (1-29):
Activates the GHRH receptor
Stimulates GH release through endogenous pituitary signaling
Does not use DAC-mediated albumin binding
Has a much shorter duration of action
Is more often discussed in research involving pulsatile GH release
Why it matters: No DAC is generally used to model shorter GHRH-like signaling, while DAC is used to study prolonged GH-axis activation.
The Main Difference: Duration of GH-Axis Signaling
The main difference between CJC-1295 DAC and No DAC is duration.
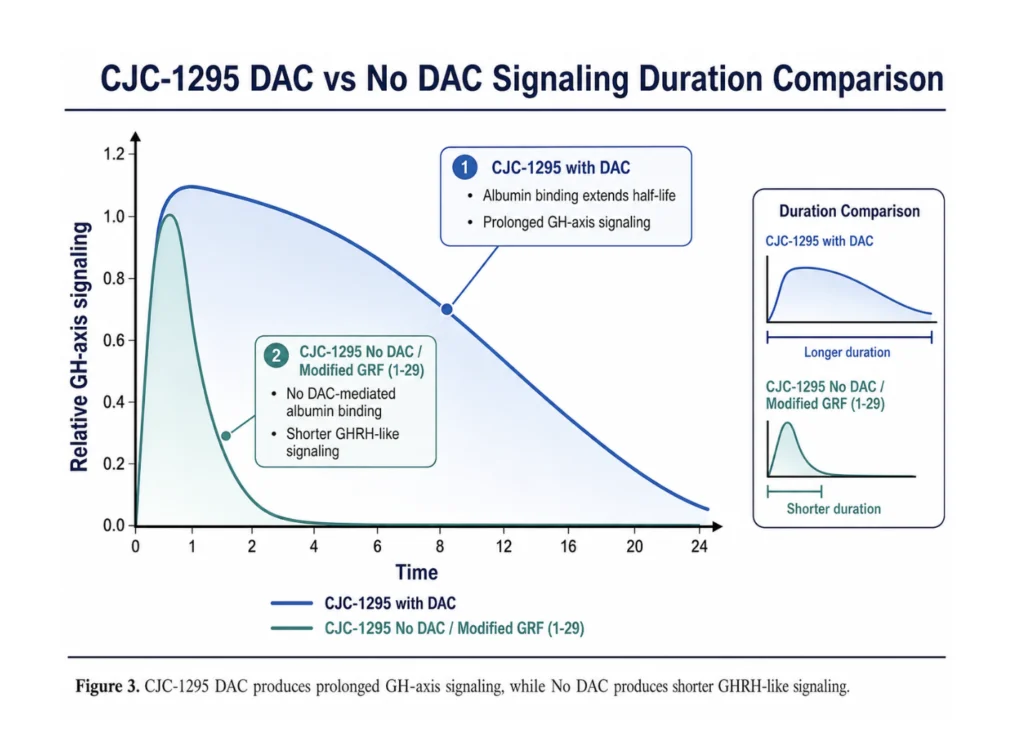
CJC-1295 DAC is long-acting because the DAC structure allows albumin binding. This extends its half-life into the range of several days in human studies.²³
CJC-1295 No DAC lacks that albumin-binding structure. As a result, it clears much faster and is associated with shorter GH pulses rather than prolonged GH/IGF-1 elevation.
In simple terms:
CJC-1295 DAC = longer acting
CJC-1295 No DAC = shorter acting
DAC changes half-life, exposure, and signaling pattern
This is why comparing the two only by name can be misleading. The presence or absence of DAC changes how the compound behaves biologically.
How Their Mechanisms Compare
Both DAC and No DAC forms act through the same primary receptor pathway:
The difference is not the receptor target. The difference is how long the signal lasts.
CJC-1295 DAC mechanism
CJC-1295 DAC activates the GHRH receptor and remains active for a longer period because of albumin binding. This produces sustained GH/IGF-1 stimulation.²
CJC-1295 No DAC mechanism
CJC-1295 No DAC activates the same receptor pathway but without extended albumin binding. This produces a shorter signal that more closely resembles a GHRH pulse.
Figure 3. CJC-1295 DAC produces prolonged GH-axis signaling, while No DAC produces shorter GHRH-like signaling.
Research Use: When Is Each Studied?
CJC-1295 with DAC
CJC-1295 DAC is most relevant when researchers want to study:
Prolonged GHRH receptor activation
Sustained GH and IGF-1 elevation
Long-duration GH-axis stimulation
Albumin-binding peptide pharmacology
Extended half-life peptide design
The original clinical studies focused on pharmacokinetics, pharmacodynamics, GH/IGF-1 response, and tolerability in healthy adults.²
CJC-1295 No DAC / Modified GRF (1-29)
No DAC is more relevant when researchers want to study:
Shorter GHRH-like signaling
Pulsatile GH release
GH-axis responsiveness
Interaction with GH secretagogues
Short-acting GHRH analog behavior
This makes No DAC conceptually closer to sermorelin-style research, though it is structurally modified for greater stability than native GHRH fragments.
Safety Considerations: DAC vs No DAC
The safety considerations are similar because both act on the GH/IGF-1 axis. However, the longer duration of DAC may create different research considerations.
Potential GH/IGF-1 pathway effects
Because both compounds stimulate GH and IGF-1 signaling, researchers often monitor outcomes related to:
Fluid retention
Edema
Glucose regulation
Tissue growth signaling
Joint discomfort or soft tissue effects
Changes in IGF-1 levels
CJC-1295 with DAC produced sustained GH and IGF-1 elevation in clinical studies, with no serious adverse reactions reported in the published trial, though the authors noted cumulative effects after repeated dosing.²
Why DAC may require extra attention
Because DAC extends exposure, it may create a longer period of GH/IGF-1 signaling. That does not automatically make it “worse,” but it does mean the research question is different.
No DAC may be preferred in models where shorter pulses are desired. DAC may be preferred when sustained stimulation is the goal.
CJC-1295 DAC vs. No DAC: Which Is “Better”?
Scientifically, neither is automatically better. They are different tools.
CJC-1295 DAC is better suited for research into long-acting GHRH analogs and sustained GH/IGF-1 elevation.
CJC-1295 No DAC is better suited for research into shorter, pulse-like GHRH receptor activation.
The choice depends on the research model, the desired duration of action, and whether the study is focused on sustained exposure or pulsatile signaling.
Why the Naming Causes Confusion
The term “CJC-1295 No DAC” is widely used commercially, but it can be confusing because CJC-1295 in the scientific literature generally refers to the DAC-containing molecule.¹²
A more chemically precise distinction is:
CJC-1295 with DAC: long-acting albumin-binding GHRH analog
Modified GRF (1-29): short-acting, no-DAC GHRH analog often sold as “CJC-1295 No DAC”
For SEO and user clarity, it is still worth using the phrase “CJC-1295 No DAC,” but the article should explain the terminology clearly.
Summary
CJC-1295 DAC and CJC-1295 No DAC are both GHRH-pathway research peptides, but they differ in one crucial feature: the presence of the drug affinity complex.
CJC-1295 with DAC binds albumin and produces sustained GH/IGF-1 signaling over multiple days. CJC-1295 No DAC lacks this albumin-binding component and is associated with shorter, more pulse-like GHRH receptor activation.
For researchers, the key question is not which one is universally better. The key question is whether the model requires prolonged GH-axis stimulation or shorter-duration GHRH signaling.
FAQs About CJC-1295 DAC vs. No DAC
What is the main difference between CJC-1295 DAC and No DAC?
The main difference is half-life. CJC-1295 DAC binds albumin through its drug affinity complex, giving it a much longer duration of action. No DAC lacks this albumin-binding component and acts for a shorter period.
Is CJC-1295 No DAC the same as Modified GRF (1-29)?
In many research peptide contexts, yes. “CJC-1295 No DAC” often refers to Modified GRF (1-29), a short-acting GHRH(1-29) analog without the DAC extension.
Does CJC-1295 DAC work differently from No DAC?
Both activate the GHRH receptor and stimulate GH release. The main difference is not receptor target, but duration: DAC produces longer GH/IGF-1 signaling, while No DAC produces shorter GHRH-like signaling.
Why does DAC make CJC-1295 last longer?
DAC allows the peptide to bind covalently to albumin, a long-lived blood protein. This protects the peptide from rapid clearance and extends its half-life.
Which is better for research: DAC or No DAC?
Neither is universally better. DAC is used when sustained GH-axis stimulation is desired. No DAC is used when shorter, pulse-like GHRH signaling is preferred.
Jetté L, Léger R, Thibaudeau K, Benquet C, Robitaille M, Pellerin I, Paradis V, van Wyk P, Pham K, Bridon D. Human growth hormone-releasing factor (hGRF)1-29 albumin bioconjugates activate the GRF receptor on the pituitary in rats: identification of CJC-1295 as a long-lasting GRF analog. Endocrinology. 2005;146(7):3052–3058.https://pubmed.ncbi.nlm.nih.gov/15817669/
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805.https://pubmed.ncbi.nlm.nih.gov/16352683/
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone persists during continuous stimulation by CJC-1295, a long-acting growth hormone-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797.https://pubmed.ncbi.nlm.nih.gov/17018654/
Sackmann-Sala L, Ding J, Frohman LA, Kopchick JJ. Activation of the GH/IGF-1 axis by CJC-1295, a long-acting GHRH analog, results in serum proteomic changes in normal adult subjects. Growth Horm IGF Res. 2009;19(6):471–477.https://pmc.ncbi.nlm.nih.gov/articles/PMC2787983/
Alba M, Fintini D, Sagazio A, Lawrence B, Castaigne JP, Frohman LA, Salvatori R. Once-daily administration of CJC-1295, a long-acting growth hormone-releasing hormone analog, normalizes growth in growth hormone-releasing hormone knockout mice. Am J Physiol Endocrinol Metab. 2006;291(6):E1290–E1294.https://pubmed.ncbi.nlm.nih.gov/16822960/
CJC-1295 vs Ipamorelin vs Sermorelin: How GH Secretagogues Compare
Disclaimer: Information provided is for research and educational purposes only. CJC-1295 is not approved by the FDA or any regulatory agency for therapeutic or cosmetic use. These compounds are not approved for human or veterinary use unless specifically noted in an approved drug context, such as tesamorelin for HIV-associated lipodystrophy.
Introduction
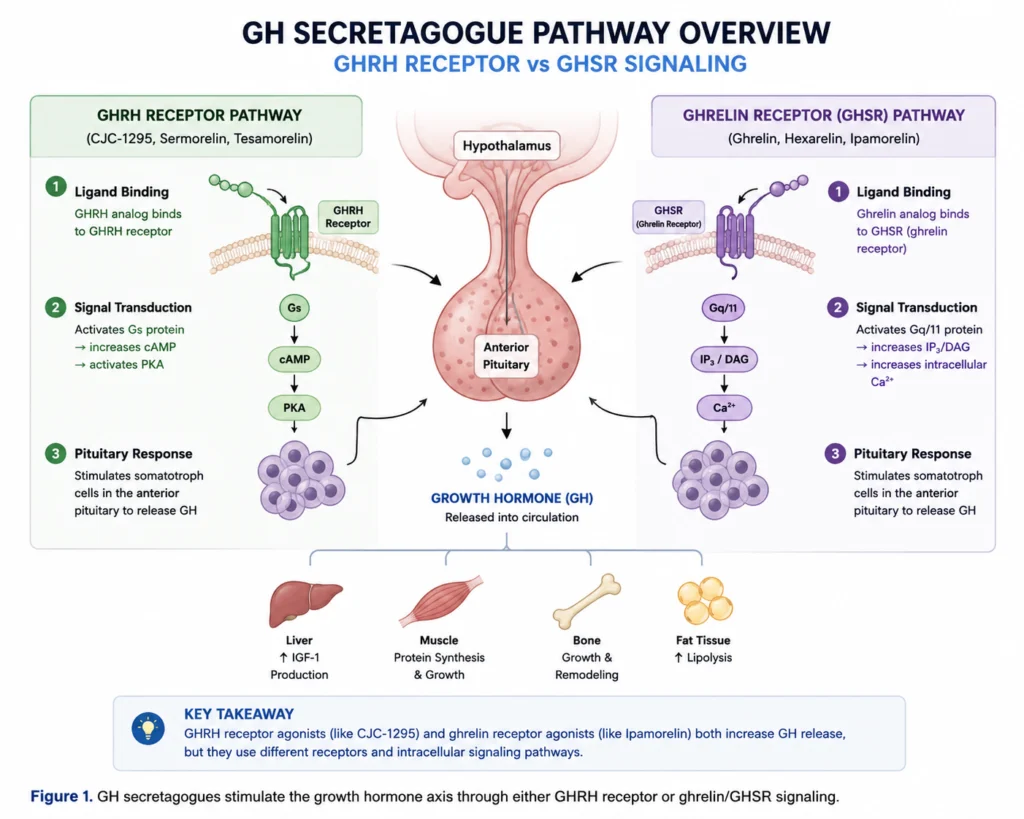
CJC-1295, Ipamorelin, and Sermorelin are often discussed together because each is studied for its relationship to the growth hormone axis. But they are not the same compound, and they do not all work through the same receptor pathway.
CJC-1295 and Sermorelin are GHRH analogs, meaning they mimic growth hormone–releasing hormone signaling at the pituitary. Ipamorelin is different: it is a growth hormone secretagogue receptor agonist, acting through the ghrelin/GHSR pathway. Other compounds in this broader research category include Tesamorelin, GHRP-2, GHRP-6, Hexarelin, and non-peptide secretagogues such as MK-677.
This article compares the major GH secretagogues by mechanism, receptor pathway, duration, research use, and how they differ from recombinant growth hormone itself.
What Are GH Secretagogues?
A growth hormone secretagogue is a compound that stimulates the body’s own growth hormone signaling rather than supplying growth hormone directly.
In research, GH secretagogues are usually grouped into two major categories:
GHRH analogs, which activate the growth hormone–releasing hormone receptor
Ghrelin/GHSR agonists, which activate the growth hormone secretagogue receptor
Both pathways can increase GH-axis activity, but they do so through different upstream signals. This matters because receptor pathway, duration, and downstream hormone patterns can vary significantly between compounds.
Quick Comparison: GH Secretagogues and Related Compounds
Compound
Category
Main Pathway
Peptide?
Key Research Distinction
CJC-1295 with DAC
GHRH analog
GHRH receptor
Yes
Long-acting GH-axis signaling via DAC/albumin binding
CJC-1295 No DAC / Modified GRF (1-29
GHRH analog
GHRH receptor
Yes
Shorter, pulse-like GHRH signaling
Sermorelin
GHRH analog
GHRH receptor
Yes
Classic GHRH(1-29) analog
Tesamorelin
GHRH analog
GHRH receptor
Yes
FDA-approved in a specific HIV-associated lipodystrophy context
Ipamorelin
GHRP / ghrelin mimetic
GHSR-1a
Yes
Selective GH secretagogue studied for GH release with limited ACTH/cortisol activity
GHRP-2
GHRP
GHSR-1a
Yes
Potent older GH secretagogue peptide
GHRP-6
GHRP
GHSR-1a
Yes
Older GHRP often associated with appetite/ghrelin-like signaling
Hexarelin
GHRP
GHSR-1a and related pathways
Yes
Potent GHRP with GH and cardiac research interest
MK-677 / Ibutamoren
Non-peptide secretagogue
GHSR-1a
No
Oral ghrelin mimetic; not a peptide
HGH / GH
Hormone
GH receptor
No
Not a secretagogue; bypasses upstream GH release pathways
Figure 1. GH secretagogues stimulate the growth hormone axis through either GHRH receptor or ghrelin/GHSR signaling
GHRH Analogs: CJC-1295, Sermorelin, and Tesamorelin
GHRH analogs mimic the natural hypothalamic signal that stimulates the pituitary gland to release growth hormone. Their primary receptor is the growth hormone–releasing hormone receptor, or GHRHR.
CJC-1295
CJC-1295 is a synthetic analog of GHRH. In the scientific literature, CJC-1295 generally refers to the DAC-modified, long-acting analog. The DAC component allows albumin binding, which extends its half-life and duration of GH-axis signaling. CJC-1295 with DAC produced sustained, dose-dependent increases in GH and IGF-1 in healthy-adult research, and GH pulsatility was reported to persist during continuous stimulation.¹²
In commercial research peptide contexts, the phrase CJC-1295 No DAC is also commonly used. This usually refers to Modified GRF (1-29), a shorter-acting GHRH analog without the albumin-binding DAC component.
Sermorelin
Sermorelin is a 29-amino-acid analog of human GHRH. It is often described as the shortest synthetic peptide with full biological activity of GHRH.³
Compared with CJC-1295 with DAC, Sermorelin is shorter acting and closer to the original GHRH(1-29) research framework. It is useful as a reference point because both Sermorelin and CJC-1295 act through the GHRH receptor.
Tesamorelin
Tesamorelin is another synthetic GHRH analog. It is especially important because it is one of the more clinically developed members of the GHRH analog family. FDA labeling for EGRIFTA WR states that tesamorelin is indicated for reducing excess abdominal fat in HIV-infected adults with lipodystrophy, while also noting that it is not indicated for weight-loss management and that long-term cardiovascular safety has not been established.⁴
For a research comparison article, Tesamorelin gives useful context: it shows that the GHRH analog category is not limited to CJC-1295 and Sermorelin.
Ghrelin/GHSR Agonists: Ipamorelin, GHRP-2, GHRP-6, and Hexarelin
The second major category is the growth hormone secretagogue receptor pathway, also known as GHSR-1a. This is the receptor system associated with ghrelin and many GH-releasing peptides.
Ipamorelin
Ipamorelin is a pentapeptide growth hormone secretagogue. In early research, it was described as the first selective GH secretagogue, showing GH-releasing potency while being more selective than older GHRPs in relation to ACTH and cortisol release.⁵
This is the reason Ipamorelin is often compared with, or paired with, CJC-1295. It works through a different upstream receptor system.
GHRP-2 and GHRP-6
GHRP-2 and GHRP-6 are older GH-releasing peptides that act through the growth hormone secretagogue receptor pathway. Studies have evaluated their GH-releasing effects in pituitary models and human endocrine settings.⁶
These compounds are useful for understanding the broader GHRP category, but from an SEO and commercial research standpoint, Ipamorelin tends to be the cleaner comparison point because it is more commonly paired with CJC-1295.
Hexarelin
Hexarelin is another potent GH secretagogue peptide. It has been studied for GH release and also appears in cardiac and metabolic research discussions. Some literature describes hexarelin as a peptide GH secretagogue with potent GH-stimulating activity and reported cardioprotective actions.⁷
Hexarelin belongs in a complete GH secretagogue overview, but it should not dominate the article unless keyword data supports a dedicated comparison page.
Non-Peptide GH Secretagogues: MK-677 / Ibutamoren
MK-677, also known as Ibutamoren, is an orally active non-peptide growth hormone secretagogue. It mimics ghrelin-like signaling at the GHSR pathway. Human research has found that MK-677 can enhance pulsatile GH secretion and increase fat-free mass over 12 months in older adults.⁸
MK-677 is relevant for topical completeness, but it is a different category from CJC-1295, Sermorelin, Tesamorelin, and Ipamorelin because it is not a peptide.
For Honest Peptide, I would include MK-677 as context rather than building the article around it.
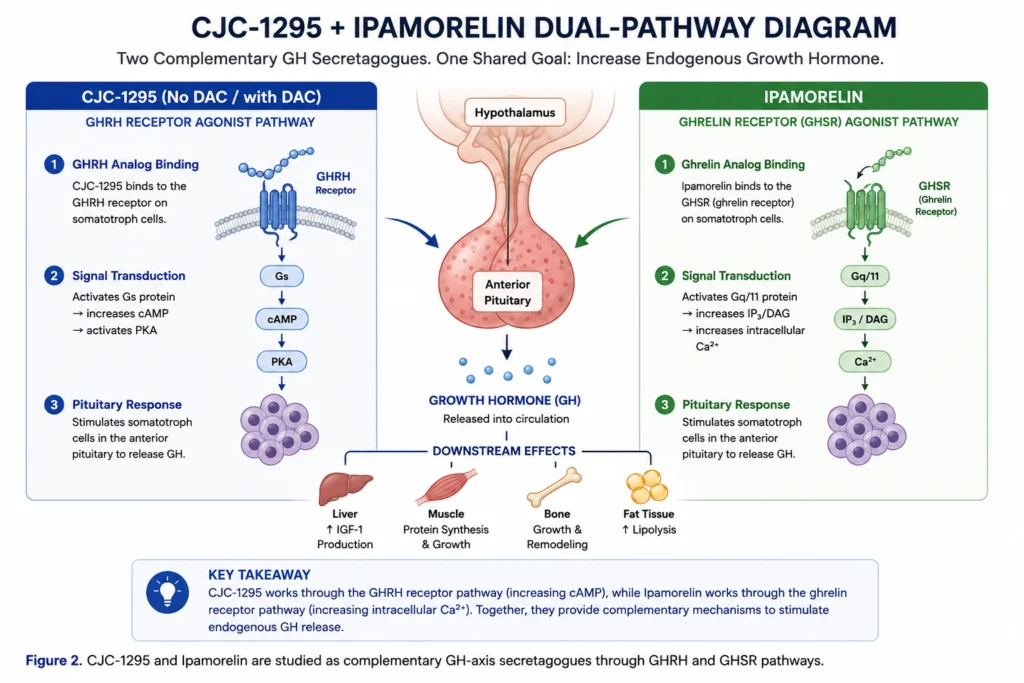
CJC-1295 + Ipamorelin: Why Are They Often Studied Together?
CJC-1295 and Ipamorelin are commonly discussed together because they represent two different upstream signals into the growth hormone axis.
CJC-1295: activates the GHRH receptor pathway Ipamorelin: activates the ghrelin/GHSR pathway
In endocrine physiology, GHRH and ghrelin-like signals can act as complementary stimulators of GH release. This is why CJC-1295 and Ipamorelin are often presented as a combination in research peptide discussions.
The key point is that they are not duplicates. They are mechanistically distinct:
Feature
CJC-1295
Ipamorelin
Class
GHRH analog
GHRP / ghrelin mimetic
Main receptor
GHRH receptor
GHSR-1a
Direct target
Pituitary somatotroph GHRHR
Ghrelin/GH secretagogue receptor
Main research role
GHRH-like GH-axis stimulation
Ghrelin-like GH secretagogue signaling
Why paired?
Provides GHRH-side signal
Provides GHSR-side signal
Why it matters: The CJC-1295 + Ipamorelin pairing is best understood as a dual-pathway GH secretagogue research model, not simply “two peptides that do the same thing.”
CJC-1295 and Sermorelin are both GHRH analogs, so this is the closest comparison in the group.
The difference is mainly duration and modification.
Sermorelin is the simpler GHRH(1-29) analog. CJC-1295, especially the DAC-modified version, was designed to extend duration through albumin binding. CJC-1295 No DAC / Modified GRF (1-29) is closer to Sermorelin in duration but includes modifications intended to improve stability.
Feature
Sermorelin
CJC-1295
Class
GHRH analog
GHRH analog
Main receptor
GHRH receptor
GHRH receptor
Duration
Shorter acting
Depends on DAC status
DAC version
No
Yes
Research distinction
Classic GHRH(1-29) analog
Modified analog; DAC form is long acting
Summary: Sermorelin is the cleaner classic GHRH analog. CJC-1295 is the more modified category, especially when DAC is present.
Ipamorelin vs Sermorelin
Ipamorelin and Sermorelin both stimulate the GH axis, but they do so through different receptors.
Sermorelin acts through the GHRH receptor. Ipamorelin acts through the growth hormone secretagogue receptor / ghrelin receptor.
This makes them mechanistically distinct even though both are grouped under GH secretagogue research.
Feature
Sermorelin
Ipamorelin
Category
GHRH analog
GHRP / ghrelin mimetic
Main receptor
GHRH receptor
GHSR-1a
Pathway
GHRH-like
Ghrelin-like
Peptide?
Yes
Yes
Main research distinction
Classic GHRH signaling
Selective GH secretagogue signaling
Summary: Sermorelin and Ipamorelin are not interchangeable. They approach the GH axis from different upstream signals.
CJC-1295 vs HGH / Growth Hormone
CJC-1295, Sermorelin, Tesamorelin, and Ipamorelin are secretagogues. They stimulate upstream pathways that can increase endogenous GH signaling.
HGH, or recombinant growth hormone, is different. It is the hormone itself.
Feature
GH Secretagogues
HGH / Recombinant GH
Acts upstream?
Yes
No
Stimulates endogenous GH release?
Yes
No
Directly activates GH receptor?
Indirectly through GH release
Yes
Preserves upstream pituitary signaling?
More relevant
Bypasses it
Research category
Secretagogue / releasing peptide
Hormone replacement model
Why it matters: Including HGH in the article helps answer common user comparisons, but it should not be the headline focus. The article is really about GH secretagogues, not direct hormone replacement.
Other GH Secretagogues: Where They Fit
A complete GH secretagogue map should include more than just CJC-1295, Ipamorelin, and Sermorelin.
GHRH analogs
These act through the GHRH receptor:
CJC-1295 with DAC
CJC-1295 No DAC / Modified GRF (1-29)
Sermorelin
Tesamorelin
Native GHRH / GRF fragments
GHRPs and ghrelin mimetics
These act through the growth hormone secretagogue receptor pathway:
Ipamorelin
GHRP-2
GHRP-6
Hexarelin
Alexamorelin / GHRP-1
MK-677 / Ibutamoren, though this is non-peptide
This section is useful for SEO because it expands the article beyond a narrow three-way comparison and establishes topical authority around the broader GH secretagogue category.
Limitations: What Does the Research Say?
Direct head-to-head comparisons between CJC-1295, Sermorelin, Ipamorelin, Tesamorelin, GHRP-2, GHRP-6, Hexarelin, and MK-677 are limited.
That matters because many online comparisons treat these compounds as interchangeable. They are not.
Key limitations:
Some compounds have direct human pharmacodynamic data.
Others rely more heavily on animal, in vitro, or older endocrine studies.
DAC and No DAC CJC-1295 are often confused.
Ipamorelin data should not be generalized to all GHRPs.
MK-677 is not a peptide and should not be treated as one.
Tesamorelin has a specific approved-drug context that does not apply to other GH secretagogues.
For scientific accuracy, each compound should be described by its receptor pathway, evidence base, and duration profile.
Summary
CJC-1295, Ipamorelin, and Sermorelin are all connected to GH-axis research, but they differ in important ways.
CJC-1295 and Sermorelin are GHRH analogs that act through the GHRH receptor. Ipamorelin is a GHSR agonist that acts through the ghrelin receptor pathway. Tesamorelin is another GHRH analog with a specific approved-drug context, while GHRP-2, GHRP-6, Hexarelin, and MK-677 belong to the broader GH secretagogue landscape.
The most important practical distinction is pathway:
This is why CJC-1295 and Ipamorelin are often studied together: they represent complementary upstream signals into GH-axis biology.
FAQs About CJC-1295, Ipamorelin, Sermorelin, and GH Secretagogues
What is the difference between CJC-1295 and Ipamorelin?
CJC-1295 is a GHRH analog that activates the GHRH receptor. Ipamorelin is a GH secretagogue peptide that activates the ghrelin/GHSR pathway. They stimulate the GH axis through different upstream receptors.
Why are CJC-1295 and Ipamorelin often combined in research?
They are often paired because CJC-1295 provides GHRH-receptor signaling while Ipamorelin provides GHSR/ghrelin-receptor signaling. This creates a dual-pathway GH secretagogue research model.
Is Sermorelin the same as CJC-1295?
No. Both are GHRH analogs, but Sermorelin is the classic GHRH(1-29) analog, while CJC-1295 is more modified. CJC-1295 with DAC has a longer duration because of albumin binding.
Is Tesamorelin a GH secretagogue?
Yes. Tesamorelin is a GHRH analog that stimulates GH-axis signaling. It also has a specific FDA-approved indication for reducing excess abdominal fat in HIV-infected adults with lipodystrophy.
Is Ipamorelin the same as GHRP-6?
No. Both act through the ghrelin/GHSR pathway, but Ipamorelin is generally discussed as more selective, while GHRP-6 is an older GH-releasing peptide often associated with appetite-related signaling.
Is MK-677 a peptide?
No. MK-677, also known as Ibutamoren, is a non-peptide oral GH secretagogue. It acts through ghrelin-like GHSR signaling but is not a peptide.
Is HGH a GH secretagogue?
No. HGH is growth hormone itself. GH secretagogues stimulate upstream signaling that can increase endogenous GH release, while HGH directly supplies the hormone.
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805. https://pubmed.ncbi.nlm.nih.gov/16352683/
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone persists during continuous stimulation by CJC-1295, a long-acting growth hormone-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797. https://pubmed.ncbi.nlm.nih.gov/17018654/
Prakash A, Goa KL. Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency. BioDrugs. 1999;12(6):419–436. https://pubmed.ncbi.nlm.nih.gov/18031173/
Raun K, Hansen BS, Johansen NL, et al. Ipamorelin, the first selective growth hormone secretagogue. Eur J Endocrinol. 1998;139(5):552–561. https://pubmed.ncbi.nlm.nih.gov/9849822/
Wu D, Chen C, Katoh K, Zhang J, Clarke IJ. The effects of GH-releasing peptide-6 and GHRP-2 on GH release. J Endocrinol. 1996. https://pubmed.ncbi.nlm.nih.gov/8699133/
Brywe KG, Leverin AL, Gustavsson M, et al. Growth hormone-releasing peptide hexarelin reduces neonatal brain injury and promotes GH secretion. Endocrinology. 2005. https://pubmed.ncbi.nlm.nih.gov/16081643/
Nass R, Pezzoli SS, Oliveri MC, et al. Effects of an oral ghrelin mimetic on body composition and clinical outcomes in healthy older adults. Ann Intern Med. 2008;149(9):601–611. https://pubmed.ncbi.nlm.nih.gov/18981485/
Sackmann-Sala L, Ding J, Frohman LA, Kopchick JJ. Activation of the GH/IGF-1 axis by CJC-1295, a long-acting GHRH analog, results in serum proteomic changes in normal
CJC-1295 is a synthetic analog of growth hormone–releasing hormone (GHRH), studied for its ability to activate the GHRH receptor, stimulate endogenous growth hormone release, and support downstream IGF-1 signaling.
Because CJC-1295 acts upstream of growth hormone, its safety profile is tied to two overlapping issues:
Peptide-specific effects, such as injection-site reactions or transient flushing
GH/IGF-1-axis effects, such as fluid retention, joint discomfort, changes in glucose handling, or other effects associated with elevated growth hormone signaling
The safety discussion is also complicated by naming. CJC-1295 with DAC is the long-acting, albumin-binding form with the strongest direct human study data. CJC-1295 without DAC, often called Modified GRF (1-29), is shorter acting and relies more heavily on broader GHRH analog and sermorelin-adjacent evidence.
This article reviews what research shows about CJC-1295 side effects, safety concerns, regulatory cautions, and the key difference between DAC and No DAC forms.
Summary Table: CJC-1295 Side Effects & Safety Data
Reported / Potential Effect
Evidence Level
Most Relevant Form
Notes
Injection-site reactions
Moderate
Mostly DAC human studies
Transient pain, swelling, and induration were among the most frequently reported events
Flushing / vasodilatory reaction
Moderate
GHRH analog class / FDA safety review
FDA has flagged systemic vasodilatory reactions among safety concerns for CJC-1295
Increased heart rate
Regulatory concern
CJC-1295 category
FDA has identified serious adverse events including increased heart rate
Headache / lightheadedness
Plausible / class-related
GHRH analog class
Fluid retention / edema
Fluid retention / edema
Reported with some GHRH analogs; not always CJC-specific
Fluid retention / edema
Fluid retention / edema
Theoretical / GH-axis related
More relevant with sustained GH/IGF-1 elevation
Common concern in GH replacement literature
Joint or muscle discomfort
Theoretical / GH-axis related
More relevant with elevated GH signaling
Seen with GH therapy and GH excess states
Carpal-tunnel-like symptoms / paresthesia
Theoretical / GH-axis related
Sustained GH/IGF-1 exposure
Known downstream GH-related safety endpoint
Glucose-handling changes
Theoretical / GH-axis related
Sustained GH/IGF-1 exposure
Relevant because GH affects insulin sensitivity and metabolic signaling
Immunogenicity / impurities
Regulatory concern
Compounded or non-pharma sources
FDA notes immunogenicity and peptide impurity concerns
Long-term safety
Limited data
Both DAC and No DAC
Long-term controlled human data are insufficient
1. Injection-Site Reactions
The most clearly reported short-term side effects in CJC-1295 research are local injection-site reactions.
In a healthy-adult study of CJC-1295 with DAC, the most frequently reported adverse events were injection-site reactions, including transient pain, swelling, and induration. The same study reported no serious adverse reactions and found sustained, dose-dependent increases in GH and IGF-1 after subcutaneous administration.
Potential local reactions include:
Redness
Mild swelling
Tenderness
Itching
Temporary discomfort
Local firmness or induration
Why it matters: Injection-site reactions appear to be the most concrete short-term adverse event signal in published CJC-1295 clinical research, especially for the DAC-modified form.
2. Flushing, Vasodilation, and Increased Heart Rate
GHRH analogs can produce transient systemic effects, including flushing or vasodilatory symptoms. This is especially important because the FDA has identified serious adverse events associated with CJC-1295, including increased heart rate and systemic vasodilatory reaction. The FDA also notes that available clinical data are limited.
Potential short-term systemic effects may include:
Facial flushing
Warmth or vasodilatory sensation
Lightheadedness
Increased heart rate
Temporary discomfort
Why it matters: These effects are not just theoretical. They have been highlighted in regulatory safety review, so they should be included clearly in any CJC-1295 safety article.
3. GH/IGF-1-Axis Related Effects
CJC-1295 stimulates the GH/IGF-1 axis rather than acting as growth hormone itself. That distinction matters, but it does not eliminate downstream GH-related safety considerations.
Human research on CJC-1295 with DAC showed sustained increases in GH and IGF-1. A related study found that CJC-1295 increased trough and mean GH secretion and IGF-1 production while preserving GH pulsatility.
Because GH and IGF-1 signaling can influence fluid balance, connective tissue, metabolism, and glucose regulation, potential GH-axis-related effects include:
Water retention
Peripheral edema
Joint stiffness or discomfort
Muscle aches
Paresthesias or tingling
Carpal-tunnel-like symptoms
Changes in insulin sensitivity or glucose handling
Adult GH replacement literature consistently identifies fluid-retention-related effects — including edema, arthralgia, carpal tunnel syndrome, and paresthesias — as common side effects of GH treatment.
Why it matters: CJC-1295 is not GH, but it is designed to increase GH-axis activity. Any safety discussion should therefore include downstream GH/IGF-1 effects as relevant endpoints.
4. DAC vs No DAC: Why Safety Profiles May Differ
The biggest safety distinction within the CJC-1295 category is duration of exposure.
CJC-1295 with DAC includes a drug-affinity-complex modification that binds albumin and extends activity. In healthy adults, DAC-modified CJC-1295 produced dose-dependent GH increases for six days or more and IGF-1 increases for nine to eleven days after a single injection; after multiple doses, mean IGF-1 remained above baseline for up to 28 days.
CJC-1295 No DAC, commonly called Modified GRF (1-29), lacks the albumin-binding extension and is shorter acting. It is more relevant to transient GHRH receptor activation rather than prolonged GH/IGF-1 exposure.
Feature
CJC-1295 with DAC
CJC-1295 No DAC / Modified GRF (1-29)
DAC extension
Yes
No
Albumin binding
Yes
No DAC-mediated binding
Duration
Long-acting
Shorter-acting
Main safety issue
Sustained GH/IGF-1 exposure
Limited direct human safety data
Strongest evidence
Human clinical studies
GHRH analog / Modified GRF / sermorelin literature
Regulatory concern
FDA has flagged CJC-1295 category safety concerns
Still affected by naming and sourcing ambiguity
Why it matters: It is not scientifically clean to copy the safety profile of DAC-modified CJC-1295 onto No DAC / Modified GRF (1-29). They share the same core receptor pathway, but their exposure profiles are different.
5. Immunogenicity, Impurities, and Product-Quality Risks
CJC-1295 safety is not only about the peptide’s intended biological mechanism. Product quality matters.
The FDA has flagged CJC-1295-related concerns including possible immunogenicity for certain routes of administration, peptide-related impurities, and API characterization complexity.
Quality-related risks may include:
Incorrect peptide identity
Peptide impurities
Endotoxin contamination
Poor sterile handling
Inaccurate concentration
Degradation from improper storage
Counterfeit or mislabeled products
Why it matters: For research peptides, safety risk can come from bad material as much as from the peptide’s intended mechanism. Third-party identity, purity, endotoxin, and contaminant testing are central to responsible research sourcing.
6. Long-Term Safety Unknowns
The available human CJC-1295 studies are limited and mostly involve the DAC-modified form. The best-known studies were short-term endocrine studies in healthy adults, measuring GH, IGF-1, pharmacokinetics, and tolerability.
Key unknowns include:
Long-term effects of repeated GH-axis stimulation
Effects of sustained IGF-1 elevation
Effects on glucose metabolism and insulin sensitivity
Cardiovascular effects in higher-risk populations
Immunogenicity after repeated exposure
Differences between DAC and No DAC safety profiles
Safety of non-pharmaceutical or poorly characterized peptide sources
Why it matters: Short-term tolerability does not equal long-term safety. This is especially true for a peptide that modulates the GH/IGF-1 axis.
Safety Profile in Research
1. No Serious Adverse Reactions in Short-Term DAC Studies
In the major healthy-adult study of CJC-1295 with DAC, no serious adverse reactions were reported. The study also found sustained, dose-dependent GH and IGF-1 increases.
This is reassuring but limited: the study was short-term and focused on healthy adults.
2. GH Pulsatility Was Preserved in DAC Research
A related CJC-1295 DAC study found that GH secretion remained pulsatile despite continuous stimulation, while trough and mean GH secretion and IGF-1 production increased.
This matters mechanistically because pulsatility is a key feature of physiologic GH signaling.
3. FDA Has Flagged CJC-1295 Safety Concerns
The FDA has identified serious adverse events associated with CJC-1295, including increased heart rate and systemic vasodilatory reaction, and has highlighted concerns about immunogenicity, peptide-related impurities, and limited clinical data.
This should be stated plainly in any safety article.
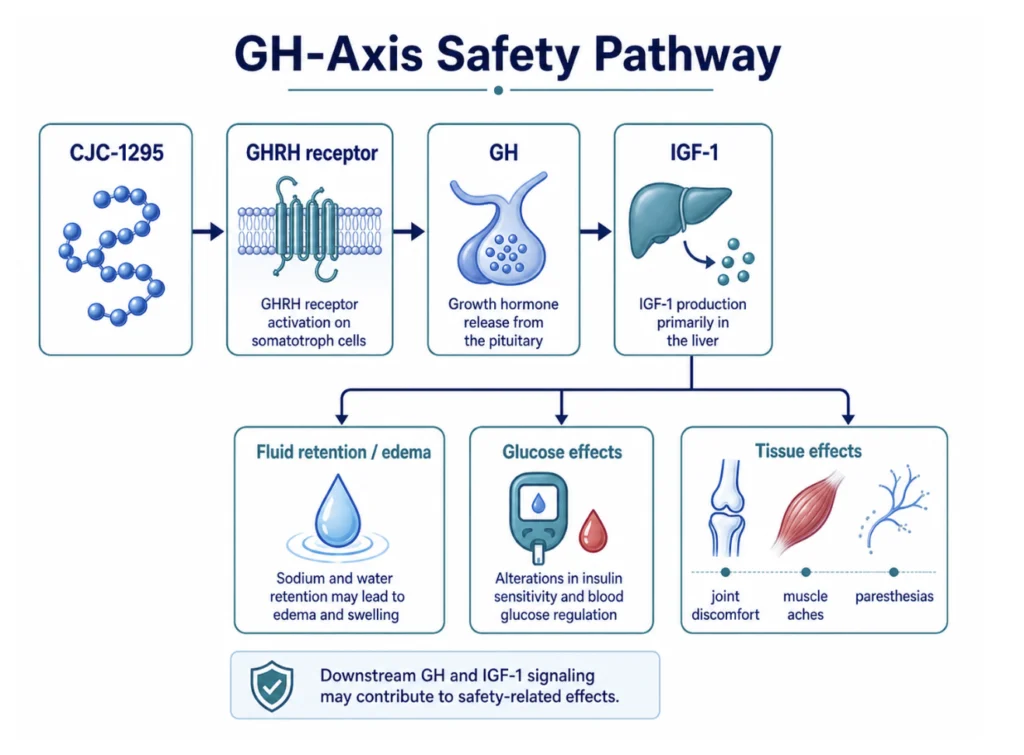
4. GH-Axis Side Effects Are Biologically Plausible
Because CJC-1295 is designed to increase GH-axis signaling, GH-related effects such as fluid retention, edema, joint discomfort, paresthesias, and carpal-tunnel-like symptoms are relevant safety endpoints, even when not proven specifically for every form of CJC-1295.
Figure 3. CJC-1295 safety considerations include downstream GH and IGF-1 pathway effects.
DAC and No DAC Are Often Confused
Searches for “CJC-1295 side effects” often mix DAC and No DAC evidence. A good safety article should clarify which form is being discussed.
Regulatory Concerns Exist
The FDA has flagged CJC-1295 for safety concerns in the compounding context, including serious adverse events and quality-control concerns.
Research Use Only
CJC-1295 is not approved for human or veterinary use and should be framed as a laboratory research peptide only.
Summary
CJC-1295’s safety profile is best understood in layers:
Published DAC studies: injection-site reactions were common; no serious adverse reactions were reported in short-term healthy-adult research.
Regulatory safety review: FDA has identified serious adverse events including increased heart rate and systemic vasodilatory reaction, and has flagged concerns around immunogenicity, impurities, and limited data.
GH-axis biology: because CJC-1295 increases GH/IGF-1 signaling, fluid retention, edema, joint discomfort, paresthesias, carpal-tunnel-like symptoms, and glucose-handling changes are relevant theoretical or downstream safety endpoints.
No DAC uncertainty: CJC-1295 No DAC / Modified GRF (1-29) is shorter acting, but direct long-term human safety evidence remains limited.
The responsible conclusion is conservative: CJC-1295 has short-term human tolerability data for the DAC form, but long-term safety remains insufficiently characterized, and regulatory agencies have raised meaningful safety and quality-control concerns..
FAQs About CJC-1295 Side Effects
What are the most common side effects of CJC-1295?
The most clearly reported side effects in published CJC-1295 DAC research are injection-site reactions, including transient pain, swelling, and induration. Other potential effects include flushing, increased heart rate, headache, lightheadedness, and GH-axis-related effects such as fluid retention or joint discomfort.
Is CJC-1295 safe?
Short-term studies of CJC-1295 with DAC reported no serious adverse reactions, but the data are limited. The FDA has identified serious adverse events associated with CJC-1295 and has raised concerns about immunogenicity, impurities, and limited clinical data.
What is the difference between CJC-1295 with DAC and No DAC for safety?
CJC-1295 with DAC is long-acting because it binds albumin and has the strongest direct human data. CJC-1295 No DAC / Modified GRF (1-29) is shorter acting, but has less direct human safety evidence. They should not be treated as identical.
Can CJC-1295 cause water retention?
Water retention is a known downstream concern with elevated GH signaling. It is not equally characterized for every form of CJC-1295, but it is a relevant safety endpoint in GH-axis research.
Does CJC-1295 increase heart rate?
The FDA has identified serious adverse events associated with CJC-1295, including increased heart rate and systemic vasodilatory reaction. This should be considered a meaningful safety concern.
Is CJC-1295 approved for human use?
No. CJC-1295 is not approved for human or veterinary use and should be described as a laboratory research peptide only.
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805.
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone persists during continuous stimulation by CJC-1295, a long-acting growth hormone-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797.
U.S. Food & Drug Administration. Certain Bulk Drug Substances for Use in Compounding That May Present Significant Safety Risks: CJC-1295.
Reed ML, Merriam GR, Kargi AY. Adult growth hormone deficiency — benefits, side effects, and risks of growth hormone replacement. Front Endocrinol (Lausanne). 2013;4:64.
Díez JJ, Sangiao-Alvarellos S, Cordido F. Treatment with growth hormone for adults with growth hormone deficiency syndrome: benefits and risks. Int J Mol Sci. 2018;19(3):893.
CJC-1295 is a synthetic analog of growth hormone–releasing hormone (GHRH), studied for its ability to activate the GHRH receptor, stimulate endogenous growth hormone signaling, and support downstream IGF-1 pathway research.¹²³
Unlike recombinant growth hormone, CJC-1295 does not supply GH directly. Instead, it acts upstream at the pituitary level, making it useful for studying the body’s own GH-regulatory system.
This article reviews the major research benefits of CJC-1295, including GH-axis activation, IGF-1 signaling, pulsatile GH secretion, body-composition research, and the key differences between DAC and No DAC forms.
Summary Table: CJC-1295 Benefits & Evidence
Benefit/ Research Area
Evidence Level
Study Type
Notes
1. GH-axis stimulation
Strong mechanistic
Human, endocrine, GHRH analog research
Activates GHRH receptor and stimulates GH release
2. IGF-1 pathway activation
Strong for DAC form
Human clinical research
CJC-1295 with DAC increased GH and IGF-1 in healthy adults
3. GH pulsatility research
Moderate
Human DAC research
GH pulsatility persisted during long-acting stimulation
4. Body-composition research
Indirect/mechanistic
GHRH analog research
Supported by broader GH/GHRH literature, not definitive CJC-specific outcome data
5. Metabolic pathway research
Indirect/mechanistic
GH/IGF-1 axis research
Relevant to lipid metabolism, substrate utilization, and endocrine signaling
6. DAC vs No DAC comparison
Strong
Pharmacologic / structural
DAC changes duration and exposure, not the core receptor pathway
1. GHRH Receptor Activation
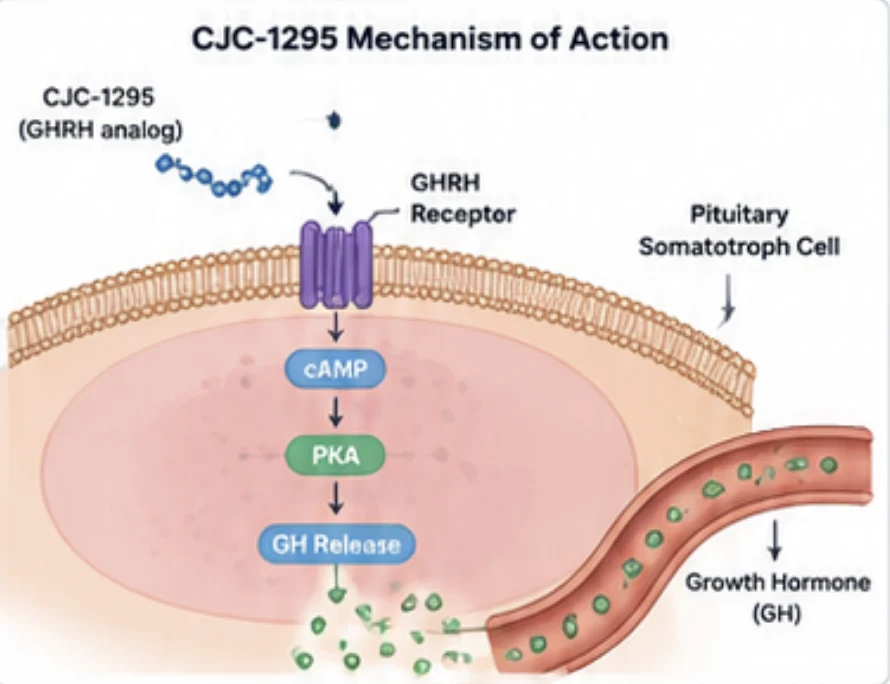
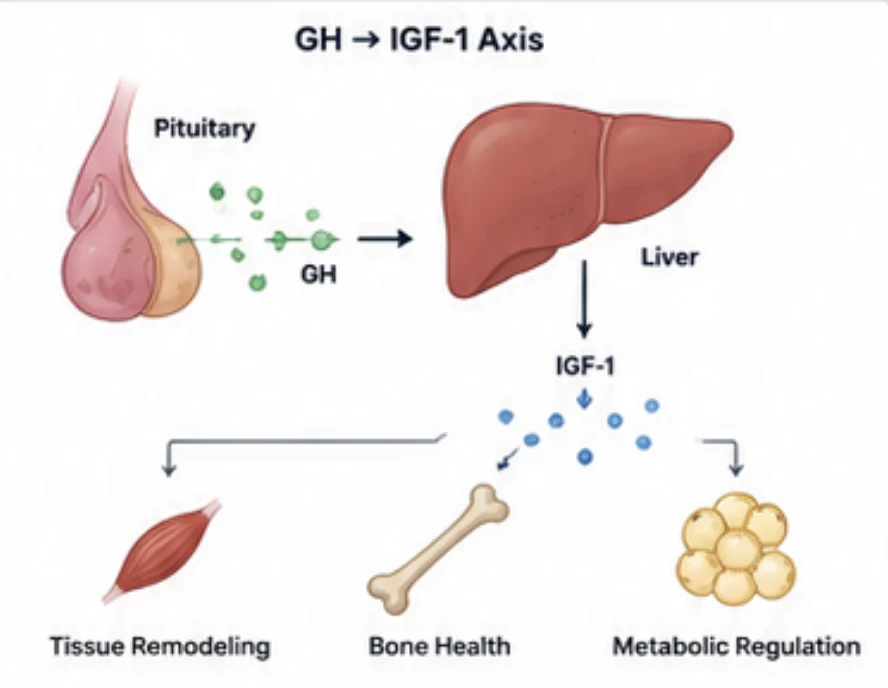
CJC-1295 binds to the growth hormone–releasing hormone receptor on pituitary somatotroph cells. This is the same receptor activated by natural GHRH, the hypothalamic peptide that controls growth hormone secretion.¹² By mimicking the active region of GHRH, CJC-1295 stimulates the pituitary through the body’s natural GH-release pathway rather than bypassing it with exogenous GH.
Why this matters: GHRH receptor activation lets researchers study GH secretion at the level of pituitary signaling, preserving the upstream control system involved in endogenous hormone release.
Figure 1. CJC-1295 activates the GHRH receptor on pituitary somatotroph cells, triggering cAMP/PKA signaling and supporting endogenous growth hormone release
2. IGF-1 Pathway Activation
Growth hormone released from the pituitary stimulates production of insulin-like growth factor 1, especially in the liver. IGF-1 is a major downstream mediator of GH signaling and is involved in anabolic signaling, tissue remodeling, and metabolic regulation.⁴⁵
In healthy-adult studies, CJC-1295 with DAC produced sustained increases in both GH and IGF-1.⁴ This is one of the strongest direct human research findings for the CJC-1295 category.
However, that evidence applies specifically to the DAC-modified long-acting form, not necessarily to CJC-1295 No DAC / Modified GRF (1-29), which has a shorter duration of action.
Why this matters: CJC-1295 connects upstream GHRH receptor activation with downstream GH/IGF-1 axis signaling.
Figure 2. Growth hormone released from the pituitary stimulates liver IGF-1 production, linking CJC-1295 research to downstream GH/IGF-1 pathway signaling
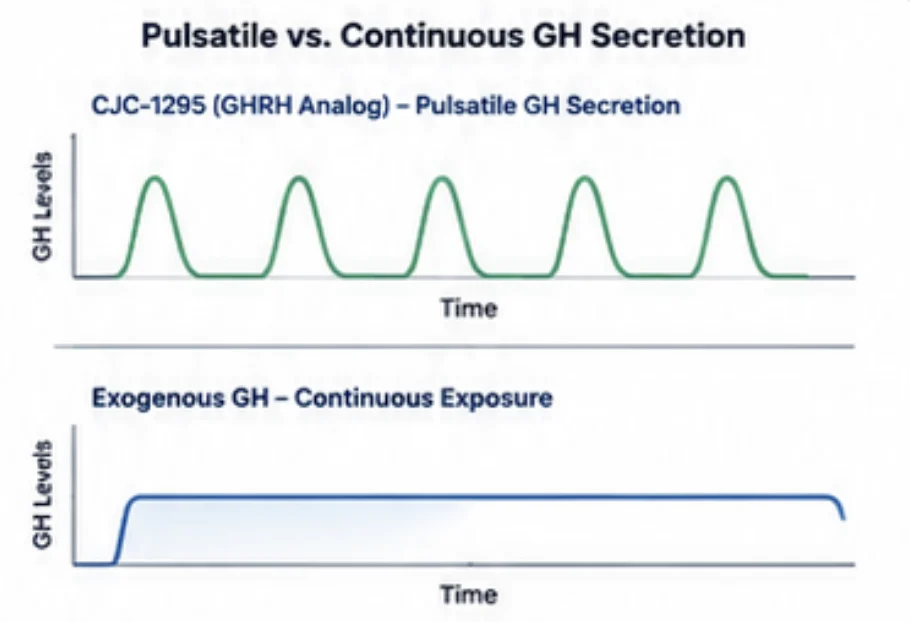
3. Pulsatile Growth Hormone Secretion
Growth hormone is naturally secreted in pulses rather than continuously. This pulsatile pattern is central to GH biology and is shaped by GHRH, somatostatin, ghrelin, sleep, age, and metabolic state.⁵⁶
One important finding from CJC-1295 with DAC research is that GH secretion remained pulsatile even during prolonged GHRH analog stimulation.⁵ This helps distinguish GHRH analogs from direct GH replacement, which bypasses upstream pituitary signaling.
Why this matters: CJC-1295 is useful for studying GH pulse dynamics, including how upstream GHRH receptor stimulation influences GH timing, amplitude, and downstream endocrine effects.
Figure 3. CJC-1295 is studied for GH-axis signaling patterns, including pulsatile growth hormone release through upstream pituitary stimulation
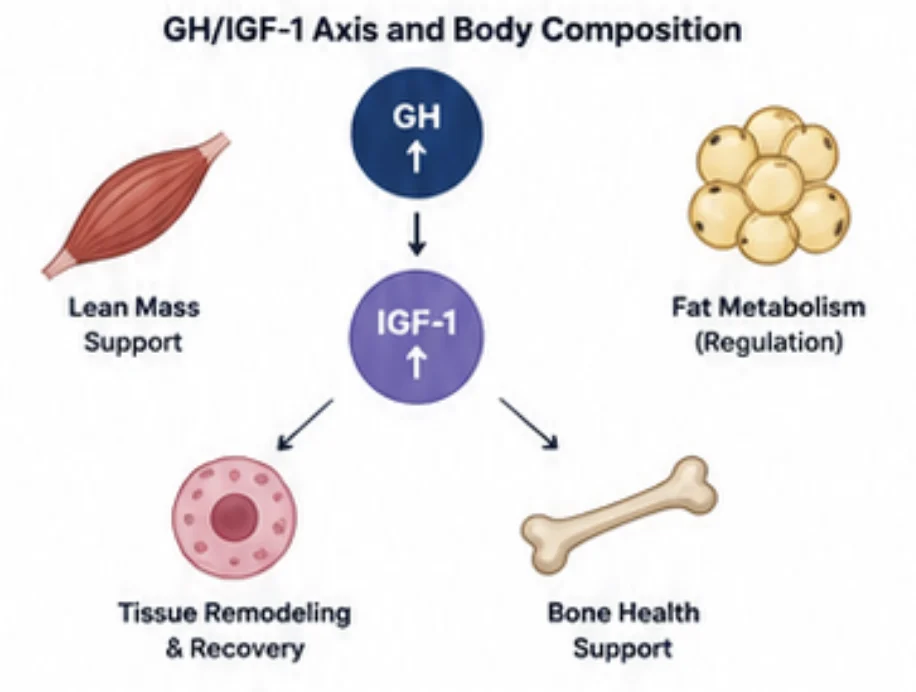
4. Body-Composition Research
The GH/IGF-1 axis is closely related to body composition, including lean tissue signaling, lipid metabolism, tissue remodeling, and age-related changes in the somatotropic axis.⁶⁷
Research on GHRH analogs, including sermorelin-related compounds, has explored effects on GH pulses, IGF-1, and lean-to-fat ratio in older adults.⁷ These findings do not directly prove body-composition benefits for all forms of CJC-1295, but they support the broader rationale for studying GHRH analogs in this area.
For CJC-1295 specifically, the most direct human evidence is endocrine: increased GH and IGF-1, particularly with the DAC-modified analog.⁴⁵
Why it matters: CJC-1295 is relevant to body-composition research because it activates a pathway involved in lean tissue signaling, fat metabolism, and tissue remodeling. Direct outcome claims should remain cautious.
Figure 4. The GH/IGF-1 axis is involved in lean tissue signaling, fat metabolism, bone health, and tissue remodeling, making it relevant to body-composition research.
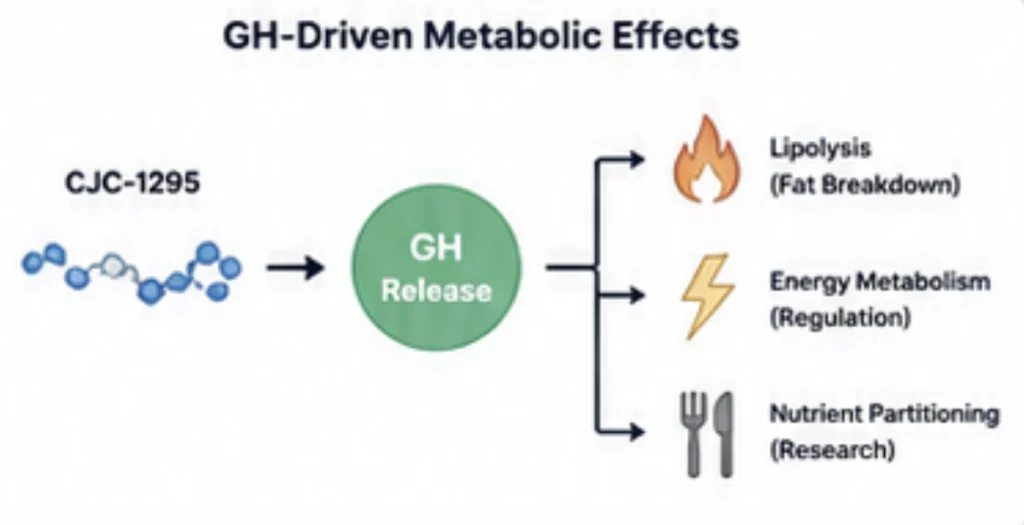
5. Metabolic and Lipolytic Pathway Research
Growth hormone influences substrate utilization, lipid mobilization, and energy metabolism. Because CJC-1295 stimulates GH-axis activity, it is relevant to research on metabolic signaling, lipolysis, and nutrient partitioning.⁶
That said, CJC-1295 should not be described as a direct fat-loss peptide. Its research relevance is upstream: it stimulates the GHRH receptor, leading to GH release and downstream endocrine effects.
Why it matters: CJC-1295 is best positioned as a GH-axis research peptide, not a direct metabolic drug. That distinction is important for scientific accuracy and compliance.
Figure 5. Through GH-axis activation, CJC-1295 is relevant to research on lipid mobilization, energy metabolism, and nutrient-partitioning pathways.
CJC-1295’s Multi-Step Endocrine Profile
Unlike peptides that act primarily on a local tissue pathway, CJC-1295 works through a coordinated endocrine cascade:
GHRH receptor activation at the pituitary
cAMP/PKA signaling inside somatotroph cells
Endogenous GH secretion
Peripheral IGF-1 production
Metabolic and anabolic pathway activation downstream
This makes CJC-1295 especially relevant in research on the GH/IGF-1 axis, pituitary signaling, and endocrine pulse dynamics.
Limitations: What Do Studies Say?
The strongest direct human data on CJC-1295 involve the DAC-modified long-acting analog, not the No DAC version.⁵⁶
For CJC-1295 without DAC, the mechanistic rationale is based on the broader GHRH (1-29), sermorelin, and Modified GRF literature.³⁴ That mechanism is biologically well grounded, but the evidence should still be described carefully.
The clean scientific distinction is:
CJC-1295 with DAC: direct clinical data showing sustained GH and IGF-1 increases
CJC-1295 No DAC / Modified GRF (1-29): shorter-acting GHRH analog used to study transient GHRH receptor activation
Both belong in the CJC-1295 research category, but claims should specify which form is being discussed.
Conclusion
CJC-1295 works by mimicking growth hormone–releasing hormone and activating the GHRH receptor on pituitary somatotroph cells. This triggers cAMP/PKA signaling, stimulates endogenous growth hormone release, and supports downstream IGF-1 pathway activation.
The key distinction is DAC status. CJC-1295 with DAC is long-acting because it binds albumin, while CJC-1295 without DAC — commonly called Modified GRF (1-29) — is shorter acting. Both forms share the same core mechanism, but they differ in duration, exposure, and research use case.
FAQs About CJC-1295 Mechanism
How does CJC-1295 stimulate growth hormone release?
CJC-1295 activates the growth hormone–releasing hormone receptor on pituitary somatotroph cells. This triggers cAMP/PKA signaling and supports endogenous growth hormone secretion.
Is CJC-1295 the same as growth hormone?
No. CJC-1295 is not growth hormone. It is a GHRH analog that stimulates the pituitary’s own growth hormone-release pathway.
What is the difference between CJC-1295 with DAC and No DAC?
CJC-1295 with DAC includes an albumin-binding drug-affinity-complex extension, making it longer acting. CJC-1295 without DAC lacks this extension and is shorter acting.
Does CJC-1295 increase IGF-1?
CJC-1295 stimulates GH release, and GH can drive downstream IGF-1 production. Human studies of CJC-1295 with DAC showed sustained increases in GH and IGF-1.
Does DAC change how CJC-1295 works?
DAC mainly changes duration of action by enabling albumin binding. The core mechanism — GHRH receptor activation followed by GH and IGF-1 signaling — remains the same.
Rivier J, Spiess J, Thorner MO, Vale W. Characterization of a growth hormone-releasing factor from a human pancreatic islet tumour. Nature. 1982;300(5889):276–278. https://pubmed.ncbi.nlm.nih.gov/6292724/
Guillemin R, Brazeau P, Bohlen P, et al. Growth hormone-releasing factor from a human pancreatic tumor that caused acromegaly. Science. 1982;218(4572):585–587. https://pubmed.ncbi.nlm.nih.gov/6812220/
Losa M, Schopohl J, von Werder K. Stimulation of GH with human GRF1-44, GRF1-40, and GRF1-29 in normal subjects. Klin Wochenschr. 1984;62(23):1109–1113. https://pubmed.ncbi.nlm.nih.gov/6240568/
Barron JL, Hopkins KD, Dunger DB, Hesp R, White A. GHRH (1-29)-NH₂ and a D-Ala² analog are potent stimulators of GH release in normal men. Clin Endocrinol (Oxf). 1985;23(4):399–407. https://pubmed.ncbi.nlm.nih.gov/2866496/
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805. https://pubmed.ncbi.nlm.nih.gov/16352683/
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone persists during continuous stimulation by CJC-1295, a long-acting growth hormone-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797. https://pubmed.ncbi.nlm.nih.gov/17018654/
The phrase “mechanism of action” refers to the biological processes through which a molecule produces its effects. In the case of CJC-1295, research demonstrates its ability to activate the growth hormone–releasing hormone receptor, stimulate pituitary growth hormone signaling, and support downstream IGF-1 pathway research.¹²³
CJC-1295 is best understood as a GHRH analog. It does not supply growth hormone directly. Instead, it mimics growth hormone–releasing hormone, the hypothalamic signal that tells the pituitary gland to release growth hormone.
The term “CJC-1295” is often used in two related but distinct ways:
CJC-1295 with DAC: the long-acting albumin-binding form originally studied in clinical research
CJC-1295 without DAC / No DAC: commonly used to describe Modified GRF (1-29), a shorter-acting GHRH analog
Both forms work through the same basic receptor system. The main difference is duration of action, not the core mechanism.
CJC-1295 Mechanism of Action: The Science Explained
CJC-1295 acts upstream of growth hormone by stimulating the body’s GH-regulatory pathway. Its mechanism can be summarized as:
Activation of the GHRH receptor
cAMP/PKA signaling inside pituitary somatotrophs
Endogenous growth hormone release
Downstream IGF-1 pathway activation
DAC-dependent differences in duration and exposure
Importantly, CJC-1295 is not growth hormone. It is a signaling peptide used to study how GHRH receptor activation influences the broader GH/IGF-1 axis.
Figure 1. CJC-1295 activates the GHRH receptor to stimulate endogenous growth hormone signaling
1. GHRH Receptor Activation
CJC-1295 binds to the growth hormone–releasing hormone receptor on pituitary somatotroph cells. This is the same receptor activated by natural GHRH, the hypothalamic peptide that controls growth hormone secretion.¹²
By mimicking the active region of GHRH, CJC-1295 stimulates the pituitary through the body’s natural GH-release pathway rather than bypassing it with exogenous GH.
Why this matters: GHRH receptor activation lets researchers study GH secretion at the level of pituitary signaling, preserving the upstream control system involved in endogenous hormone release.
2. cAMP/PKA Signaling in Pituitary Somatotrophs
Once CJC-1295 activates the GHRH receptor, the receptor stimulates adenylate cyclase, increasing cyclic AMP and activating protein kinase A.³⁴
This cAMP/PKA pathway is central to GHRH-mediated growth hormone release. It drives intracellular signaling events that support GH synthesis and secretion from pituitary somatotroph cells.Why this matters: This makes CJC-1295 useful for studying how receptor-level stimulation produces measurable endocrine output through the GH axis.
3. Endogenous Growth Hormone Release
The direct endocrine result of GHRH receptor activation is increased growth hormone release from the pituitary. Unlike recombinant GH, CJC-1295 does not replace GH directly; it stimulates the system that regulates GH secretion.³⁵
Growth hormone is naturally secreted in pulses, shaped by GHRH, somatostatin, ghrelin, sleep, age, and metabolic status. One important finding from CJC-1295 with DAC research is that GH secretion remained pulsatile even during prolonged stimulation.⁶
Why this matters: GH pulsatility is central to normal growth hormone biology. CJC-1295 is valuable in research because it activates the upstream signaling pathway rather than simply adding GH from outside the system.
4. Downstream IGF-1 Pathway Activation
Growth hormone released from the pituitary acts on peripheral tissues, especially the liver, to stimulate production of insulin-like growth factor 1. IGF-1 is a major downstream mediator of GH-axis activity and is involved in anabolic signaling, tissue remodeling, and metabolic regulation.⁵⁶
In healthy-adult studies, CJC-1295 with DAC produced sustained increases in both GH and IGF-1.⁵ These data apply specifically to the long-acting DAC-modified form, but they help explain why CJC-1295-class peptides are used to study GH/IGF-1 pathway activation.
Why this matters: CJC-1295 is not only relevant to GH release itself; it is also used to study how upstream GHRH receptor activation affects downstream IGF-1 signaling.
5. DAC and Duration of Action
The biggest mechanistic distinction within the CJC-1295 category is DAC status.
CJC-1295 with DAC includes a drug-affinity-complex modification that allows the peptide to bind circulating albumin. This extends exposure and produces a longer-acting GH/IGF-1 stimulation profile.⁵⁶
CJC-1295 without DAC, commonly called Modified GRF (1-29), lacks this albumin-binding extension. It is shorter acting and more relevant to research models focused on transient GHRH receptor activation.
Feature
CJC-1295 with DAC
CJC-1295 No DAC / Modified GRF (1-29)
Primary receptor
GHRH receptor
GHRH receptor
DAC extension
Yes
No
Albumin binding
Yes
No DAC-mediated binding
Duration profile
Long-acting
Shorter-acting
Main pathway
GHRHR → cAMP/PKA → GH → IGF-1
GHRHR → cAMP/PKA → GH → IGF-1
Research use
Sustained GH/IGF-1 stimulation
Transient GH-axis signaling
Why this matters: DAC changes how long CJC-1295 remains active. It does not fundamentally change the receptor pathway. Both forms work through GHRH receptor activation, but they create different exposure profiles.
CJC-1295’s Multi-Step Endocrine Profile
Unlike peptides that act primarily on a local tissue pathway, CJC-1295 works through a coordinated endocrine cascade:
GHRH receptor activation at the pituitary
cAMP/PKA signaling inside somatotroph cells
Endogenous GH secretion
Peripheral IGF-1 production
Metabolic and anabolic pathway activation downstream
This makes CJC-1295 especially relevant in research on the GH/IGF-1 axis, pituitary signaling, and endocrine pulse dynamics.
Limitations: What Do Studies Say?
The strongest direct human data on CJC-1295 involve the DAC-modified long-acting analog, not the No DAC version.⁵⁶
For CJC-1295 without DAC, the mechanistic rationale is based on the broader GHRH (1-29), sermorelin, and Modified GRF literature.³⁴ That mechanism is biologically well grounded, but the evidence should still be described carefully.
The clean scientific distinction is:
CJC-1295 with DAC: direct clinical data showing sustained GH and IGF-1 increases
CJC-1295 No DAC / Modified GRF (1-29): shorter-acting GHRH analog used to study transient GHRH receptor activation
Both belong in the CJC-1295 research category, but claims should specify which form is being discussed.
Conclusion
CJC-1295 works by mimicking growth hormone–releasing hormone and activating the GHRH receptor on pituitary somatotroph cells. This triggers cAMP/PKA signaling, stimulates endogenous growth hormone release, and supports downstream IGF-1 pathway activation.
The key distinction is DAC status. CJC-1295 with DAC is long-acting because it binds albumin, while CJC-1295 without DAC — commonly called Modified GRF (1-29) — is shorter acting. Both forms share the same core mechanism, but they differ in duration, exposure, and research use case.
FAQs About CJC-1295 Mechanism
How does CJC-1295 stimulate growth hormone release?
CJC-1295 activates the growth hormone–releasing hormone receptor on pituitary somatotroph cells. This triggers cAMP/PKA signaling and supports endogenous growth hormone secretion.
Is CJC-1295 the same as growth hormone?
No. CJC-1295 is not growth hormone. It is a GHRH analog that stimulates the pituitary’s own growth hormone-release pathway.
What is the difference between CJC-1295 with DAC and No DAC?
CJC-1295 with DAC includes an albumin-binding drug-affinity-complex extension, making it longer acting. CJC-1295 without DAC lacks this extension and is shorter acting.
Does CJC-1295 increase IGF-1?
CJC-1295 stimulates GH release, and GH can drive downstream IGF-1 production. Human studies of CJC-1295 with DAC showed sustained increases in GH and IGF-1.
Does DAC change how CJC-1295 works?
DAC mainly changes duration of action by enabling albumin binding. The core mechanism — GHRH receptor activation followed by GH and IGF-1 signaling — remains the same.
Rivier J, Spiess J, Thorner MO, Vale W. Characterization of a growth hormone-releasing factor from a human pancreatic islet tumour. Nature. 1982;300(5889):276–278. https://pubmed.ncbi.nlm.nih.gov/6292724/
Guillemin R, Brazeau P, Bohlen P, et al. Growth hormone-releasing factor from a human pancreatic tumor that caused acromegaly. Science. 1982;218(4572):585–587. https://pubmed.ncbi.nlm.nih.gov/6812220/
Losa M, Schopohl J, von Werder K. Stimulation of GH with human GRF1-44, GRF1-40, and GRF1-29 in normal subjects. Klin Wochenschr. 1984;62(23):1109–1113. https://pubmed.ncbi.nlm.nih.gov/6240568/
Barron JL, Hopkins KD, Dunger DB, Hesp R, White A. GHRH (1-29)-NH₂ and a D-Ala² analog are potent stimulators of GH release in normal men. Clin Endocrinol (Oxf). 1985;23(4):399–407. https://pubmed.ncbi.nlm.nih.gov/2866496/
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805. https://pubmed.ncbi.nlm.nih.gov/16352683/
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone persists during continuous stimulation by CJC-1295, a long-acting growth hormone-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797. https://pubmed.ncbi.nlm.nih.gov/17018654/
The Growth Hormone–Releasing Peptide That Mimics the Body’s Own GHRH
Disclaimer: Information provided is for research and educational purposes only. Sermorelin is not approved by the FDA or any regulatory agency for therapeutic or cosmetic use.
Introduction
CJC-1295 is a synthetic analog of growth hormone–releasing hormone (GHRH), the natural hypothalamic peptide that signals the pituitary gland to release growth hormone (GH).¹²
It was developed as part of a broader effort to create longer-lasting and more stable GHRH analogs for studying GH secretion, IGF-1 signaling, and age-related changes in the somatotropic axis.³⁴
The name “CJC-1295” is often used in two ways. Technically, CJC-1295 refers to the long-acting DAC-modified analog designed to bind albumin and extend activity. In research and commercial settings, however, the term is also commonly used for CJC-1295 without DAC, also called Modified GRF (1-29) — a shorter-acting GHRH analog based on the active 1-29 region of GHRH.
GH-axis signaling, pituitary stimulation, GH pulse dynamics, IGF-1 pathway research
Two common forms
CJC-1295 with DAC and CJC-1295 without DAC
Key distinction
DAC-modified CJC-1295 is long-acting; No DAC / Modified GRF (1-29) is shorter-acting
Not the same as GH
CJC-1295 stimulates endogenous GH release rather than supplying growth hormone directly
Chemical Structure
CJC-1295 is based on the active 1-29 amino-acid region of human GHRH. This region contains the core sequence required for GHRH receptor activation and growth hormone release.³⁴
The long-acting form, CJC-1295 with DAC, includes structural substitutions designed to improve stability, along with a drug-affinity-complex modification that enables albumin binding. This albumin-binding feature extends the compound’s half-life and produces a longer GH/IGF-1 signaling profile.⁵⁶
By contrast, CJC-1295 without DAC, commonly called Modified GRF (1-29), lacks the albumin-binding DAC component. It is still a modified GHRH analog, but it behaves as a shorter-acting research compound.
In simple terms: both forms are GHRH analogs, but the DAC version is engineered for extended circulation, while the No DAC version is built around shorter GHRH-like receptor activation.
Figure 1: CJC-1295 chemical structure
How CJC-1295 Works (In Brief)
CJC-1295 works by mimicking GHRH and activating the GHRH receptor on pituitary somatotroph cells. This triggers intracellular cAMP/PKA signaling, which stimulates endogenous growth hormone release from the pituitary.³⁴
Growth hormone then acts on peripheral tissues, especially the liver, to support production of insulin-like growth factor 1 (IGF-1), a major downstream mediator of GH-axis activity.The key point is that CJC-1295 is not growth hormone. It acts upstream by stimulating the body’s GH-release pathway. The DAC form extends this signaling through albumin binding, while the No DAC form is shorter acting and more pulse-like.
Discovery & Research Milestones
The scientific background of CJC-1295 begins with the discovery of human growth hormone–releasing hormone in the early 1980s. Researchers identified GHRH from human pancreatic tumor tissue associated with acromegaly, then confirmed its sequence and biological activity.¹²
This discovery led to the development of shorter active GHRH fragments, including GHRH (1-29)-NH₂, later known as sermorelin. Researchers found that the first 29 amino acids of GHRH retained much of the hormone’s GH-releasing activity.³⁴
CJC-1295 was developed later as a more durable GHRH analog. The DAC-modified version was designed to extend biological activity through albumin binding, allowing researchers to study longer-duration GH and IGF-1 signaling.⁵⁶
Year
Study & Source
Key Finding
1982
Rivier J et al., Nature
Identified human growth hormone–releasing factor from pancreatic tumor tissue.¹.
1982
Guillemin R et al., Science
Independently confirmed the human GHRH sequence.²
1984–1985
Losa M; Barron J et al.
Established GHRH (1-29)-NH₂ and related analogs as potent GH secretagogues.³⁴
1990s
Modified GRF development
Amino-acid substitutions were explored to improve stability of GHRH (1-29)-based analogs.
2006
Teichman SL et al., JCEM
Long-acting CJC-1295 with DAC produced sustained GH and IGF-1 increases in healthy adults.⁵
2006
Ionescu M & Frohman LA, JCEM
GH secretion remained pulsatile during continuous stimulation by CJC-1295 with DAC.⁶
2009
Sackmann-Sala L et al., Clinical Cancer Research
Used CJC-1295-induced GH/IGF-1 axis activation to study downstream serum biomarkers.⁸
What Research Shows
Growth Hormone Stimulation
CJC-1295 acts upstream of the growth hormone itself. Instead of supplying GH directly, it activates the GHRH receptor on pituitary somatotroph cells, stimulating intracellular cAMP/PKA signaling and supporting endogenous GH release.³⁴
This makes CJC-1295 useful for studying how the pituitary responds to GHRH-like stimulation and how GH output affects downstream endocrine pathways.
IGF-1 Pathway Activation
Growth hormone released from the pituitary stimulates production of insulin-like growth factor 1 (IGF-1), especially in the liver. IGF-1 is one of the major downstream mediators of GH activity and is involved in anabolic signaling, tissue remodeling, and metabolic regulation.
In healthy-adult studies, long-acting CJC-1295 with DAC produced sustained increases in GH and IGF-1.⁵ Those findings apply specifically to DAC-modified CJC-1295, but they help explain why CJC-1295-class peptides are used in GH/IGF-1 axis research.
Preservation of GH Pulsatility
GH is naturally released in pulses, not as a flat continuous signal. One important finding from CJC-1295 DAC research is that GH secretion remained pulsatile even during extended stimulation.⁶
That matters because pulsatility is central to normal GH biology. It also helps distinguish GHRH analogs from direct GH replacement, which can create less physiologic exposure patterns.
Short-Acting vs. Long-Acting Research Models
The biggest practical distinction within the CJC-1295 category is whether the peptide includes DAC.
CJC-1295 with DAC is designed for longer exposure and sustained GH/IGF-1 stimulation. CJC-1295 without DAC, or Modified GRF (1-29), is shorter acting and more relevant to studies of transient GHRH receptor activation.
Both are GHRH analogs, but they should not be treated as interchangeable.
CJC-1295 With DAC vs. CJC-1295 No DAC
Feature
CJC-1295 with DAC
CJC-1295 No DAC / Modified GRF (1-29)
Technical identity
Original long-acting CJC-1295
Modified GRF (1-29), commonly called CJC-1295 No DAC
DAC extension
Yes
No
Albumin binding
Yes
No DAC-mediated binding
Duration profile
Long-acting
Shorter-acting
Main research use
Sustained GH/IGF-1 stimulation
Transient GHRH receptor activation
GH secretion pattern
Sustained elevation with pulsatility preserved in studies
Pulse-like GHRH analog research
Best description
Long-acting GHRH analog
Short-acting modified GHRH analog
The cleanest way to explain it: CJC-1295 with DAC is the long-acting albumin-binding version; CJC-1295 No DAC is the shorter-acting Modified GRF (1-29) version.
CJC-1295 belongs to the same broad GHRH analog family as sermorelin. Both are based on the active 1-29 region of GHRH and both stimulate the pituitary through the GHRH receptor.
The main difference is structural. Sermorelin is the simpler GHRH (1-29)-NH₂ fragment, while CJC-1295-related analogs include modifications designed to improve stability and duration.
Feature
Sermorelin
CJC-1295
Core identity
GHRH (1-29)-NH₂
Modified GHRH analog
Primary target
GHRH receptor
GHRH receptor
Main effect
Endogenous GH release
Endogenous GH release
Duration
Short-acting
Depends on DAC status
DAC version available
No
Yes
Research focus
GH testing, GH pulse physiology
GH-axis signaling, IGF-1 pathway research, sustained or transient stimulation models
Sermorelin is best understood as the simpler first-generation GHRH fragment, while CJC-1295 represents a more modified class of GHRH analogs.
Read more about CJC vs Sermorelin and other GH-secretogues here
Summary
CJC-1295 is a synthetic GHRH analog used to study the growth hormone axis. It works by activating the GHRH receptor on pituitary somatotrophs, stimulating endogenous GH release and downstream IGF-1 signaling.
The most important distinction is DAC status. CJC-1295 with DAC is the long-acting albumin-binding version originally developed to extend GHRH activity. CJC-1295 without DAC, commonly called Modified GRF (1-29), is shorter acting and used in research models focused on transient GHRH receptor activation.
In both forms, CJC-1295 remains scientifically relevant because it allows researchers to study GH-axis regulation upstream of growth hormone itself.¹–⁸
FAQs About CJC-1295
What is CJC-1295?
CJC-1295 is a synthetic analog of growth hormone–releasing hormone, or GHRH. It is studied for its ability to activate the GHRH receptor, stimulate endogenous growth hormone release, and support downstream IGF-1 signaling.
Is CJC-1295 the same as growth hormone?
No. CJC-1295 is not growth hormone. It acts upstream by stimulating the pituitary gland’s own growth hormone release pathway, while growth hormone itself acts directly through the GH receptor.
What is CJC-1295 used for in research?
CJC-1295 is used in research on GH-axis signaling, pituitary stimulation, growth hormone pulse dynamics, IGF-1 pathway activation, and the effects of GHRH analogs on endocrine signaling.
What is the difference between CJC-1295 with DAC and CJC-1295 No DAC?
CJC-1295 with DAC includes a drug-affinity-complex modification that enables albumin binding and extends its duration of action. CJC-1295 No DAC, commonly called Modified GRF (1-29), lacks this albumin-binding component and is shorter acting.
Is CJC-1295 No DAC the same as Modified GRF (1-29)?
In most research peptide contexts, yes. “CJC-1295 No DAC” is commonly used to refer to Modified GRF (1-29), a shorter-acting modified GHRH analog without the DAC albumin-binding extension.
How does CJC-1295 work?
CJC-1295 works by activating the GHRH receptor on pituitary somatotroph cells. This triggers intracellular cAMP/PKA signaling, stimulates growth hormone release, and supports downstream IGF-1 signaling.
Is CJC-1295 the same as Sermorelin?
No. Both are GHRH analogs, but Sermorelin is the simpler GHRH (1-29)-NH₂ fragment. CJC-1295 is a more modified GHRH analog, and the DAC version is designed for longer duration through albumin binding.
Does CJC-1295 increase IGF-1?
CJC-1295 can support downstream IGF-1 signaling by stimulating growth hormone release. Human studies of CJC-1295 with DAC reported sustained increases in both GH and IGF-1, but those findings apply specifically to the DAC-modified form.
Why is the name CJC-1295 confusing?
The name is confusing because scientific literature generally uses CJC-1295 to refer to the DAC-modified, long-acting analog. In commercial research peptide discussions, “CJC-1295 No DAC” is often used to describe Modified GRF (1-29), which is related but shorter acting.
Rivier J, Spiess J, Thorner MO, Vale W. Characterization of a growth hormone-releasing factor from a human pancreatic islet tumour.Nature. 1982;300(5889):276-278. https://pubmed.ncbi.nlm.nih.gov/6292724/
Guillemin R, Brazeau P, Bohlen P, et al. Growth hormone-releasing factor from a human pancreatic tumor that caused acromegaly.Science. 1982;218(4572):585-587. https://pubmed.ncbi.nlm.nih.gov/6812220/
Losa M, Schopohl J, von Werder K. Stimulation of GH with human GRF1-44, GRF1-40, and GRF1-29 in normal subjects. Klin Wochenschr. 1984;62(23):1109–1113. https://pubmed.ncbi.nlm.nih.gov/6240568/
Barron JL, Hopkins KD, Dunger DB, Hesp R, White A. GHRH (1-29)-NH₂ and a D-Ala² analog are potent stimulators of GH release in normal men. Clin Endocrinol (Oxf). 1985;23(4):399–407. https://pubmed.ncbi.nlm.nih.gov/2866496/
Teichman SL, Neale A, Lawrence B, Gagnon C, Castaigne JP, Frohman LA. Prolonged stimulation of growth hormone and insulin-like growth factor I secretion by CJC-1295, a long-acting analog of GH-releasing hormone, in healthy adults. J Clin Endocrinol Metab. 2006;91(3):799–805. https://pubmed.ncbi.nlm.nih.gov/16352683/
Ionescu M, Frohman LA. Pulsatile secretion of growth hormone persists during continuous stimulation by CJC-1295, a long-acting growth hormone-releasing hormone analog. J Clin Endocrinol Metab. 2006;91(12):4792–4797. https://pubmed.ncbi.nlm.nih.gov/17018654/
Soule S, et al. Incorporation of D-Ala² in growth hormone-releasing hormone (1-29)-NH₂: effects on metabolic clearance and biological activity. Clin Endocrinol (Oxf). 1994. https://pubmed.ncbi.nlm.nih.gov/7962295/
Disclaimer: All information presented in this article is strictly for scientific, academic, and educational purposes. Research peptides discussed here are intended solely for laboratory research and in vitro studies. They are not approved by the FDA or any regulatory agency for human or veterinary use, clinical applications, therapeutic use, or consumption of any kind.
“Research peptides” are synthetic or isolated peptide sequences manufactured strictly as laboratory reagents—not pharmaceuticals. They sit in a specific regulatory category known as Research Use Only (RUO). Legally, RUO peptides are chemical tools for experiments — not drugs, not supplements, and not products for treating people.
This distinction governs everything: how they’re manufactured, what testing is expected, and what vendors are allowed to claim. RUO peptides are evaluated on chemical quality (sequence, purity, solubility), not clinical safety (sterility, viral clearance, validated cleaning).
For a Principal Investigator, Lab Manager, or anyone sourcing research-use-only peptides, understanding the RUO framework is essential for three reasons:
Legal Compliance: Ensures reagents are used strictly within FDA boundaries (typically in vitro assays or regulated laboratory animal studies).
Experimental Integrity: Distinguishes between “chemically clean enough for a petri dish” (RUO) and “manufactured for human safety” (GMP).
Vendor Credibility: Clarifies which suppliers operate as true scientific vendors vs. gray-market sellers who misuse RUO labels while making illegal therapeutic claims.
This guide maps the RUO landscape so you can evaluate suppliers, interpret documentation, and understand exactly what RUO peptides are—and what they are not designed for.
2. RUO Classification and Legal Framework
The RUO designation is defined by FDA guidance, which separates laboratory-use chemicals from diagnostic or therapeutic products. The defining feature of a compliant RUO peptide is its labeling, which functions as a regulatory firewall.
FDA Expectation is that products not approved for human diagnostic or therapeutic use should carry statements such as:
“For Research Use Only. Not for use in diagnostic or therapeutic procedures.”
This labeling exempts a product from the pre-market approval required for drugs as long as the vendor stays within permitted marketing boundaries.
Permitted Claims:
Chemical identity
Sequence accuracy
Solubility
Purity metrics
General assay utility
Prohibited Claims:
Dosage protocols
Disease-treatment or health-benefit statements
Any implication of human administration
Testimonials describing physiological effects
If a vendor labels a product “RUO” while simultaneously hinting at muscle recovery, weight loss, or healing, they are misbranding an unapproved drug. That exposes both seller and buyer to regulatory risk.
For a deeper breakdown of RUO labeling, intended use, and FDA enforcement history, see our RUO Legal Framework Pillar [LINK]
3. Research Peptides vs. GMP vs. Clinical-Grade (RUO vs GMP vs Clinical)
“Research peptides,” “GMP peptides,” and “clinical-grade peptides” are often chemically identical — the difference lies in the manufacturing process, not the sequence itself.
A. Research Use Only (RUO)
Environment: Standard lab or ISO 9001 facility
Quality Focus: Product quality — purity and correct sequence
Documentation: COA showing purity + identity
Cost: Low to moderate
B. cGMP (Current Good Manufacturing Practice)
Environment: FDA-audited cleanrooms with validated environmental controls
Quality Focus: Process control — sterility, traceability, batch reproducibility
Documentation: Full batch records, cleaning validation, viral clearance logs
Cost: Often 10x–50x RUO pricing
C. Clinical Grade
Definition: GMP material approved for use under an IND or equivalent
Requirement: Entire manufacturing history must be GMP-compliant
Key Takeaway: A peptide cannot be “upgraded” from RUO to GMP by additional testing. The manufacturing history defines the regulatory category.
4. Appropriate Applications (RUO Only)
RUO peptides are designed for laboratory experiments, not human or veterinary use. They are foundational tools in early-stage discovery and analytical chemistry.
Valid Applications:
Assay Development: ELISA standards, Western blots, calibration curves
Mass Spectrometry Calibration: Peptide reference standards
Invalid Applications:
Any form of human administration
Therapeutic or aesthetic purposes
Diagnostics or clinical decision-making
Veterinary treatment
Reputable suppliers enforce these boundaries explicitly (“Not for Human Consumption”) and sell only into controlled laboratory environments.
5. How RUO Status Shapes Testing Requirements
Because RUO peptides are not evaluated by the FDA for human safety, the agency does not prescribe specific QC standards. In practice, quality varies by vendor, and testing is the primary differentiator between professional suppliers and gray-market sellers.
High-quality RUO testing focuses on three core metrics:
A. Purity (Chemical Cleanliness)
Evaluated via High-Performance Liquid Chromatography (HPLC).
Standard for general research: ≥95%
Standard for sensitive assays: ≥98%
Quality signal: A single sharp dominant peak with minimal baseline noise
B. Identity (Sequence Confirmation)
Verified via Mass Spectrometry (ESI-MS or MALDI-TOF).
Observed molecular weight must match theoretical MW (±1 Da)
Prevents the “99% pure but wrong sequence” problem
Critical for publication-grade work
C. Contaminants (Endotoxins & Residual Solvents)
Not legally mandated for RUO, but essential for reliable biological data.
Endotoxins: Lipopolysaccharides that can distort cell-culture assays. Some higher-end suppliers screen for levels such as <0.25 EU/mg
Heavy Metals: Trace contamination (e.g., Pb, Cd, Hg, As) can interfere with enzymatic assays and cytotoxicity screens. High-end suppliers run ICP-MS panels to confirm levels within acceptable research thresholds (often <0.5–1.0 ppm total)
Residual Solvents: TFA, acetonitrile, and other synthesis agents should be minimized. High-end QC includes solvent analysis for cytotoxicity reduction
Key Takeaway: In the RUO market, data is your only insurance. If a vendor cannot provide batch-specific purity, identity, and contaminant metrics, you’re buying a mystery powder.
6. The Research-to-Clinical Continuum
Peptide development progresses through defined stages:
Discovery (RUO)
Fast, inexpensive synthesis
Screening dozens–hundreds of candidates
Pre-Clinical (High-Grade RUO / GLP)
Stricter QC
Endotoxin control and validated methods
Clinical (GMP)
Fresh synthesis under full GMP
Sterility, viral clearance, validated cleaning, full traceability
Common Misconception: A peptide advertised as “99% pure” RUO is still not safe for human use. Purity only measures chemical cleanliness, not sterility, viral safety, or GMP compliance.
7. How to Evaluate Research Peptide Vendors
The online peptide market is unregulated and often deceptive. Marketing adjectives like “Ultra Premium” or “Pharma Grade” are meaningless. Only data matters.
A. The COA Test
A trustworthy vendor provides a batch-specific COA for the exact lot being shipped.
Red Flag:
Sample/generic COAs
No lot number
No testing lab named
B. Data Visibility (Show Your Work)
Good: Full HPLC chromatograms + MS spectra for the exact batch
Bad: Typed summaries like “Purity: 99%” with no raw data
C. Responsiveness and Technical Transparency
A credible supplier answers technical questions with technical answers.
A storefront with questionable QC will be unable to do so.
8. Common Misuses + Marketplace Confusion
“Lifestyle peptides” (BPC-157, Semaglutide, TB-500, etc.) created a gray market where sellers abuse RUO labels to evade drug laws.
“Research peptides” that look like consumer products
Researchers should avoid vendors prioritizing biohackers. They rarely maintain documentation, QC, or compliance required for reproducibility.
9. Summary & Related Articles
Research peptides are chemical tools defined by the RUO framework. Strictly laboratory-use, never for humans, and evaluated on chemical—not clinical—criteria. High-quality RUO peptides rely on:
HPLC purity data
MS identity confirmation
Transparent COAs
Honest, compliant marketing
10. Related Articles
Explore the rest of our other Pillar Pieces in our Research Hub:
How Are Peptides Made? [LINK HERE] Step-by-step guide to how peptides are made: SPPS, cleavage, HPLC purification, lyophilization, and QC so you can interpret COAs and compare RUO suppliers.
How to Read a Peptide COA? [LINK HERE] Learn how to read a peptide COA the right way—HPLC purity, MS identity, net peptide content, and digital verification—to separate real analytical data from marketing.
Definitive Guide to Peptide Storage & Stability [LINK HERE] Practical SOP for peptide storage, reconstitution, and aliquoting. Understand degradation pathways and keep RUO peptides stable and sterile.
How to Select a Peptide Vendor [LINK HERE] Tips on how to select a peptide vendor: due diligence checklist for RUO peptides, transparency, COA quality, cold chain, pricing, and marketing red flags.
11. FAQs
Can a 99% pure RUO peptide be used in humans?
No. Purity ≠ sterility, viral clearance, or GMP documentation. RUO peptides are not manufactured for human use.
What is “Net Peptide Content”?
The fraction of the powder that is actual peptide (excluding salts and water). A 10 mg vial may contain ~7–8 mg peptide + 2–3 mg of excipients. This is normal.
What differentiates two vendors both selling “99% purity” peptides?
COA legitimacy, batch specificity, third-party testing, documentation quality, and consistency. Purity alone is not a differentiator.
Are RUO peptides regulated by the FDA?
They are not pre-market regulated like drugs, but RUO products are subject to labeling and misbranding laws. The FDA defines the boundaries for permitted claims.
Do I need a COA for every vial?
You need a COA for every lot number. A single COA covers all vials from that synthesis batch.
References
U.S. Food and Drug Administration. Distribution of In Vitro Diagnostic Products Labeled for Research Use Only or Investigational Use Only: Guidance for Industry and FDA Staff. November 2013. Accessed November 19, 2025.
Vincent Balgos. “An Introduction to Research Use Only (RUO).” Jama Software Blog, June 2025.
Joanne S. Hawana and Benjamin M. Zegarelli. “FDA Warning Letter Is a Stark Reminder That If You Claim Your Product Is RUO, It Has to Be RUO.” Mintz Insights, April 3, 2024.
Johnathon D. Anderson, PhD. “Certified Peptides: A Complete Scientific Guide to Authentic, Verified Research-Grade Peptides.” Peptide Systems Blog, October 8, 2024.
Johnathon D. Anderson, PhD. “What ‘Premium’ Really Means and How to Choose a Trusted Peptide Supplier.” Peptide Systems Blog, 2025.
Dr. Numan S. “Certificates of Analysis for Peptides: What Researchers Need to Know.” Verified Peptides Knowledge Hub, August 7, 2025.
FDA Warning Letter to USApeptide.com. “Notice of Unlawful Sale of Unapproved and Misbranded Drugs” (MARCS-CMS 696885). February 26, 2025.
Matthew Perrone. “A Closer Look at the Unapproved Peptide Injections Promoted by Influencers and Celebrities.” AP News, July 13, 2023.
How Lab-Grade Peptides Are Manufactured (SPPS → Purification → Lyophilization)
Disclaimer: All information presented in this article is strictly for scientific, academic, and educational purposes. Research peptides discussed here are intended solely for laboratory research and in vitro studies. They are not approved by the FDA or any regulatory agency for human or veterinary use, clinical applications, therapeutic use, or consumption of any kind.
1. Introduction
“Research peptides” are synthetic or isolated peptide sequences manufactured strictly as Lab-grade peptide manufacturing is a precision chemical workflow that transforms raw amino acids into high-purity research reagents.
Unlike pharmaceutical production—which centers on sterility, validated fill-finish, and patient safety—the Research Use Only (RUO) process focuses on chemical purity, sequence fidelity, and reproducibility.
The core goal: A chemically verified peptide, typically ≥95% pure and often 98–99% for sensitive assays.
The manufacturing pipeline follows a clean, linear “assembly line” logic:
Solid-Phase Peptide Synthesis (SPPS): Build the chain on a resin bead.
Cleavage & Deprotection: Release the peptide as crude material.
Purification (RP-HPLC): Remove deletion variants and related impurities.
Lyophilization: Freeze-dry into a stable powder.
Quality Control & Packaging: Verify identity and purity, then seal for shipment.
Understanding this process helps researchers interpret Certificates of Analysis (COAs), anticipate solubility behavior, and identify differences between RUO and GMP manufacturing.
2. Step 1: Solid-Phase Peptide Synthesis (SPPS)
Solid-Phase Peptide Synthesis is the universal standard for manufacturing research peptides. It builds the peptide like a tower—one amino acid at a time—anchored to a solid resin bead.
How SPPS Works
Anchoring: The first amino acid (C-terminus) is bonded to an insoluble polymer resin.
The Fmoc Cycle: Repeated automated cycles assemble the chain:
Deprotect: Remove the Fmoc protective group.
Couple: Add the next amino acid.
Wash: Rinse away unreacted reagents.
Repeat: This cycle repeats until the full sequence is built.
Why SPPS Matters
Because the peptide stays attached to a solid support, excess reagents and by-products are easily washed away.
However, incomplete couplings create deletion variants (peptides missing one residue). These cannot be washed out and must be removed later during purification.
Modern synthesizers automate the entire process, improving coupling efficiency and batch reproducibility.
Once the chain is fully assembled, it must be removed from the resin and stripped of its side-chain protections.
The Cleavage Reaction
The Cleavage Reaction
Manufacturers expose the peptidyl-resin to a strong acid cocktail, typically:
Trifluoroacetic Acid (TFA)
Scavengers (to neutralize reactive intermediates)
The Result
A crude peptide solution containing:
The intended peptide
Deletion sequences
Truncated fragments
Residual synthesis chemicals
Most research peptides become TFA salts here, because the amines in the peptide bind to TFA during cleavage.
4. Step 3: Peptide Purification by RP-HPLC
The crude material now contains a mix of “right” and “almost-right” peptides. Purification via Reversed-Phase High-Performance Liquid Chromatography (RP-HPLC) isolates the correct sequence.
How RP-HPLC Works
Injection:
The crude mixture is loaded onto a hydrophobic silica column.
The target peptide elutes at a specific retention time.
Fraction Collection:
UV absorbance identifies the main peak.
That fraction is collected; impurities are discarded.
Purity Outcome
HPLC purification typically boosts purity from 30–70% (crude) to:
≥95% standard
98–99% for sequences that purify cleanly
This step is the primary determinant of final research-grade peptide quality..
5. Step 4: Peptide Lyophilization (Freeze-Drying)
After purification, the peptide is dissolved in a solvent mixture that must be removed without heating.
The Lyophilization Steps
Freeze:
Rapid deep-freezing at ~–80°C.
Vacuum:
Pressure is dropped to near-vacuum.
Sublimation:
Ice transitions directly to vapor, leaving the peptide behind.
The Result
A fluffy, white or off-white anhydrous powder, highly stable in dry form.
Stability note: Many peptides remain stable for years at –20°C, but sequences containing Met, Cys, or Trp are more oxidation-prone and may slowly degrade even when lyophilized.der. [LINK TO STORAGE PILLAR]
6. Step 5: Quality Control & COA Generation
Before release, each batch undergoes analytical testing to verify identity and purity. These data populate the COA.
The Two Essential QC Tests
Mass Spectrometry (Identity)
Confirms molecular weight matches theoretical mass within tight tolerance.
Validates that the sequence is correct (no missing/extra residues).
Analytical HPLC (Purity)
Reports the percent area of the main peak vs impurities.
Net Peptide Content
Purity ≠ weight.
A lyophilized powder contains peptide plus:
Counter-ions (e.g., TFA)
Residual water
Example:
A “10 mg” vial may contain ~8 mg peptide and ~2 mg salts/water.
This is normal for all lyophilized RUO peptides.e.
7. Packaging, Salt Form, and Storage
Packaging
Glass vials are standard to prevent adsorption.
Vials are often purged with nitrogen or argon to displace moisture and oxygen.
Labels include batch number, purity, mass, and RUO disclaimer.
Storage
Store lyophilized peptides at –20°C (or colder for long-term stability).
Always allow the closed vial to warm to room temperature before opening to avoid condensation.
Salt Form
Most RUO peptides are TFA salts due to the cleavage step.
Some researchers prefer alternative counter-ions (e.g., acetate, HCl) for specific assay compatibility; reputable suppliers can provide these forms on request.
8. Summary
Lab-grade peptide manufacturing is a deliberate, multi-step chemical process focused on purity, identity, and reproducibility.
While the molecules may be chemically identical to pharmaceutical peptides, the RUO workflow lacks sterility, GMP documentation, and clinical validation—making them inappropriate for human use.
9. Related Articles
Explore the rest of our other Pillar Pieces in our Research Hub:
What are Research Peptides? [LINK HERE] Learn what research peptides are under the FDA RUO framework, how they differ from GMP/clinical material, and what that means for legality, QC, and lab use.
How to Read a Peptide COA? [LINK HERE] Learn how to read a peptide COA the right way—HPLC purity, MS identity, net peptide content, and digital verification—to separate real analytical data from marketing.
Definitive Guide to Peptide Storage & Stability [LINK HERE] Practical SOP for peptide storage, reconstitution, and aliquoting. Understand degradation pathways and keep RUO peptides stable and sterile.
How to Select a Peptide Vendor [LINK HERE] Tips on how to select a peptide vendor: due diligence checklist for RUO peptides, transparency, COA quality, cold chain, pricing, and marketing red flags.
10. FAQs
What’s the difference between “crude” and “purified” peptides?
Crude: 30–70% pure, full of deletion fragments and by-products. Purified: ≥95% pure after RP-HPLC.
Are RUO peptides sterile?
No.RUO peptides are manufactured under clean chemical-reagent conditions, not sterile GMP conditions.Sterility, endotoxin validation, and aseptic fill-finish only apply to clinical-grade materials.
Does lyophilization alter peptide performance?
Lyophilization generally preserves chemical integrity by limiting moisture and degradation pathways. However, reconstitution protocol and solvent choice matter—especially for hydrophobic or aggregation-prone sequences.
Q: Why does the vial look empty or contain only a film of powder?
1 mg or 5 mg of dry peptide is microscopic. Lyophilized cakes often collapse into a thin film.Let the powder settle at the bottom before opening.
Why is my peptide a “TFA salt”?
During cleavage, TFA protonates basic residues, forming TFA salts. This is standard across the industry. Alternative salt forms can be provided upon request for certain research needs.
References
U.S. Food and Drug Administration. Distribution of In Vitro Diagnostic Products Labeled for Research Use Only or Investigational Use Only: Guidance for Industry and FDA Staff. November 2013. Accessed November 19, 2025.
Vincent Balgos. “An Introduction to Research Use Only (RUO).” Jama Software Blog, June 2025.
Joanne S. Hawana and Benjamin M. Zegarelli. “FDA Warning Letter Is a Stark Reminder That If You Claim Your Product Is RUO, It Has to Be RUO.” Mintz Insights, April 3, 2024.
Johnathon D. Anderson, PhD. “Certified Peptides: A Complete Scientific Guide to Authentic, Verified Research-Grade Peptides.” Peptide Systems Blog, October 8, 2024.
Johnathon D. Anderson, PhD. “What ‘Premium’ Really Means and How to Choose a Trusted Peptide Supplier.” Peptide Systems Blog, 2025.
Dr. Numan S. “Certificates of Analysis for Peptides: What Researchers Need to Know.” Verified Peptides Knowledge Hub, August 7, 2025.
FDA Warning Letter to USApeptide.com. “Notice of Unlawful Sale of Unapproved and Misbranded Drugs” (MARCS-CMS 696885). February 26, 2025.
Matthew Perrone. “A Closer Look at the Unapproved Peptide Injections Promoted by Influencers and Celebrities.” AP News, July 13, 2023.
Understanding and interpreting a Certificate of Analysis (COA): A Researcher’s Field Guide
Disclaimer: All information presented in this article is strictly for scientific, academic, and educational purposes. Research peptides discussed here are intended solely for laboratory research and in vitro studies. They are not approved by the FDA or any regulatory agency for human or veterinary use, clinical applications, therapeutic use, or consumption of any kind.
1. Introduction
A Certificate of Analysis (COA) is the single most important document in the research peptide supply chain. It transforms an unlabeled white powder into a scientifically verifiable reagent.
For Research Use Only (RUO) peptides—materials that are not approved for human or veterinary use—the COA is your primary quality assurance tool. Because RUO peptides are not regulated like pharmaceuticals, the burden of verification sits with the researcher. A legitimate COA must answer four core questions:
Identity – Is this the correct sequence? (Mass Spectrometry)
Purity – Is it chemically clean? (HPLC)
Content – How much actual peptide is present? (Net Peptide Content)
Contaminants – Are there any harmful compounds also present? (Heavy Metals, Endotoxins)
Credible suppliers use independent, third-party laboratories to generate COAs. Third-party testing eliminates conflict of interest and gives the researcher unbiased, empirical data—not marketing claims.
Note: Most 3rd Party providers group identity, purity and content into a single test result (e.g., Janoshik, annotated below). Contaminants usually require separate tests – typically 1 test for endotoxins and 1 for heavy metals.
2. HPLC Purity — The “Cleanliness” Check
High-Performance Liquid Chromatography (HPLC) is the standard method for quantifying peptide purity. It separates the target peptide from peptide-related impurities (deletion sequences, truncated fragments, and synthesis by-products).
What the Purity Percentage Actually Means
The COA will list a purity value such as 98.7%. This represents:
(Area of the target peak) ÷ (Total area of all UV-absorbing peptide-related peaks)
Important nuance:
HPLC purity reflects only UV-absorbing organic impurities, not water, salts, or non-chromophore contaminants. This is why purity and Net Peptide Content differ.
How to Interpret It
≥99% — Excellent. Ideal for quantitative assays, structural biology, binding studies, or sensitive cell work.
95–98% — Standard RUO grade. Suitable for most discovery-phase research.
<95% — Potentially problematic for precision assays.
Chromatogram or No Chromatogram?
Some labs (e.g., Janoshik) provide numerical purity reports without chromatogram images. Others attach full chromatograms. A lack of chromatogram does not invalidate the results, rather it is a function of how they present results to customers. However, as a best practice we recommend asking a new tester for the chromatogram file to ensure it matches what they have provided in the test result.
3. Mass Spectrometry — The “Identity” Check
HPLC cannot confirm sequence identity. A peptide missing one amino acid may appear 99% pure on HPLC, but would be 0% the desired peptide.
Mass Spectrometry (MS) is the only reliable way to confirm identity.
Most 3rd party testers provide both MS & HPLC in a single test and will only alert you in the event that Mass Spec does not detect the correct sequence. As a best practice, always confirm that your tester is providing MS.
4. Net Peptide Content — The “Missing Mass”
This is the most misunderstood metric in peptide QC. And unfortunately no tester does this well.
Purity vs. Net Content
Purity = peptide content vs. peptide impurities
Net Peptide Content = peptide vs. everything else (water + salts + counter-ions)
A peptide can be 99% pure yet 70–85% net content. This is because HPLC only captures peptide related content, and therefore the 1% residual is composed only of peptide-related impurities. It fails to capture anything non-peptide related.
Why Net Content Is Always <100%
Lyophilized peptides bind mutiple forms of non-peptide content, including:
Residual moisture (hygroscopic behavior, especially Lys/Arg-rich sequences)
Counter-ions (TFA, Acetate, HCl)
Atmospheric water during freeze-drying transfer
Practical Impact
If you dissolve a 5 mg vial assuming all 5 mg is active peptide, your molar concentration will be incorrect.
Example:
Gross weight: 5 mg
Net content: 80%
Actual peptide mass: 4 mg
Always adjust dosing based on net content when performing precise quantitative work.
Where Testers Fall Short
Most testers provide net peptide content in their results. However, they do not provide gross peptide content. As a result it is impossible to calculate the gross-to-net ratio (net weight/gross weight) and thereby not possible to ascertain how much non-peptide content is contained in the product
This is mostly harmless as most residue (TFA, residual moisture) is benign. However, there is harmful non-peptide content, which must be screened for. This is where contaminant testing comes into play.
5. Contaminant Testing — Filtering out Harmful Compounds
When evaluating peptide quality, most people focus on purity (HPLC) and identity (mass spec). Those confirm you have the correct molecule and that it’s relatively clean from peptide-related byproducts.
However, there is a separate and equally important category: Non-peptide contaminants
Two of the most important are heavy metals and endotoxins.
Heavy Metals
Heavy metals are trace inorganic elements that can enter the product during:
Raw material sourcing
Manufacturing equipment contact
Poorly controlled synthesis environments
The primary metals typically screened are Lead (Pb), Cadmium (Cd), Mercury (Hg), Arsenic (As).
Heavy metals are invisible to HPLC and mass spec and, if present, will accumulate in organic matter offer time with negative effects on neurological, renal and hepatic function.
It is therefore crucial to test for heavy metals; accordingly, Honest Peptide tests for every single product for heavy metals.
The standard method for heavy metals testing is ICP-MS (Inductively Coupled Plasma Mass Spectrometry), which detects metals as parts-per-billion (ppb) levels. The primary metals screened are Lead (Pb), Cadmium (Cd) and Arsenic (As)
The test output is typically delivered as a binary detected or not detected, but a legitimate tester should also be able to produce metal-by-metal quantitative detail upon request.
Summary Results(Janoshik)
Detailed Results(Janoshik) – UPON REQUEST
Endotoxins
Endotoxins are Lipopolysaccharides (LPS) from the outer membrane of Gram-negative bacteria. They are not “live bacteria” but fragments of bacterial cell walls. They can enter peptides if:
Water systems are not properly controlled
Manufacturing environments lack sterility
Filtration steps are inadequate
As they are not live bacteria, endotoxins will not cause any kind of infection. However, sustained exposure can trigger immune reactions leading to fever and inflammation.
The standard method for endotoxin testing is LAL Test (Limulus Amebocyte Lysate assay). This assay detects endotoxin activity at very low levels and reports results in EU/ml (Endotoxin Units per milliliter) or in some cases EU/vial.
Some 3rd party labs provide the results of the assay as a binary pass/fail. Others provide an exact EU number.
Example of Binary Pass/Fail Test
5. How to Evaluate Claims — The “Trust But Verify” Model
In RUO peptides, data is everything. A static PDF alone is not enough.
1. Digital Verification (Required)
Top-tier analytical labs provide:
Verification Keys
COA IDs
QR codes
Database lookup portals
A legitimate COA must be verifiable directly on the lab’s server. Further, a serious researcher must verify the COA on the 3rd party testers website. Otherwise, it is very easy for unscrupulous suppliers to photoshop results. Indeed, we see this all the time
2. Technical Transparency
A credible vendor is clear about:
Salt form (TFA vs Acetate)
Net peptide content
Purity measurement method
Identity verification method
Where the testing was performed
Opaque suppliers should be treated with caution.
6. RUO vs. GMP — Managing Expectations Accurately
A COA for a Research Use Only peptide is not:
A sterility certificate
A pyrogen (endotoxin) certificate
A GMP batch record
Evidence of suitability for human use
FDA-reviewed documentation
RUO COAs Contain:
Sequence identity (MS)
Chemical purity (HPLC)
Net content
Physical description
RUO COAs Do Not Contain:
Sterility testing (unless test is added)
Endotoxin testing (unless test is added)
Bioburden testing
Viral or microbial safety data
GMP compliance statements
Clinical suitability assessments
7. What a COA Cannot Tell You (Important for Research Planning)
A COA cannot determine:
Whether your peptide is sterile
Whether the material is free of pyrogens
How the peptide should behave biologically
Whether impurities are biologically benign
How stable the peptide will be after reconstitution
Whether the vendor followed GMP manufacturing controls
These limitations apply to the entire RUO category, not just a specific supplier.
8. Summary
A peptide COA is your primary quality assurance document.
To evaluate a peptide, confirm:
HPLC Purity — How clean is it?
Mass Spec Identity — Is the sequence correct?
Net Peptide Content — How much peptide is actually present?
Non Peptide Contaminants – Heavy Metals & Endotoxins
Digital Verification – Always cross-check COAs on 3rd Party lab website
9. Related Articles
Explore the rest of our other Pillar Pieces in our Research Hub:
What are Research Peptides? [LINK HERE] Learn what research peptides are under the FDA RUO framework, how they differ from GMP/clinical material, and what that means for legality, QC, and lab use.
How Are Peptides Made? [LINK HERE] Step-by-step guide to how peptides are made: SPPS, cleavage, HPLC purification, lyophilization, and QC so you can interpret COAs and compare RUO suppliers.
Definitive Guide to Peptide Storage & Stability [LINK HERE] Practical SOP for peptide storage, reconstitution, and aliquoting. Understand degradation pathways and keep RUO peptides stable and sterile.
How to Select a Peptide Vendor [LINK HERE] Tips on how to select a peptide vendor: due diligence checklist for RUO peptides, transparency, COA quality, cold chain, pricing, and marketing red flags.
10. FAQs
How do I verify a third-party COA?
Use the verification key, QR code, or database lookup. If unsure, email the testing lab with the Report ID.
Why is there no batch number on my vial?
RUO products often omit vial-level batch IDs. The COA itself is the batch record.
How do I verify a third-party COA?
Use the verification key, QR code, or database lookup. If unsure, email the testing lab with the Report ID.
What should I do if purity is <98%?
For exploratory work it may be acceptable, but for quantitative assays impurities can skew results. If the purity is lower than advertised, contact the vendor.
Does the COA guarantee endotoxins or sterility testing?
No. RUO COAs do not include endotoxin or sterility testing, although these are occasionally added on by RUO vendors.
References
Bachem. “Quality Control of Amino Acids & Peptides: A Guide.” 2025.
Numan, S. “Certificates of Analysis for Peptides: What Researchers Need to Know.” Verified Peptides, 2025.
United States Pharmacopeia (USP). General Chapter <1043>. 2021.
You must be over 21 to visit this site. By clicking “Yes”, you confirm that you are 21 years of age or older, agree that any products purchased will be used strictly for research purposes and accept our Terms of Service.